This is the third installation of my journal from the day I was first diagnosed with cancer of the bladder. These are my thoughts, my prayers, my observations and my journey as I navigate this brave new world. Read more about it in this post called “My Journey with Cancer (Pt 3.)”
My journey with cancer (Part 3). It is 4:15 a.m. and for the last hour I have been adding to my blog. If you click on the home page or the title to this webpage (www.watch-fire.net), you’ll find over 150 posts on current events, geopolitics, psychology and science as well as book reviews, expositions to certain Biblical passages, word studies, etc. At the moment, I am writing about Down Syndrome in children and how these children fit into the tile of life and the fabric of the Kingdom. I am continuing to journal about Russia’s nuclear policy and the odds of Russia resorting to nuclear weapons in the Ukraine war. Also, I’m researching the simplicity of the Gospel and I’m about to start a post on Pulitzer Prize winner John Steinbeck. I thank Deena for encouraging me to retire from teaching, else I’d be grading essays instead. I’ve had thirty-five years of that! And speaking of Deena, thank you all for the kind words and encouragement that Deena received from her post last weekend. I hope she will continue to share her thoughts and feeling about cancer, and if anyone has a personal story to share about cancer, I’ll be glad to include it in this blog as well. Just send it to: gangof4@verizon.net.
At the moment, it is snowing outside, and we expect close to half of a foot in town. Dee and I ran to the store yesterday, so we’ll be staying home, as snug as bugs in a rug.
Today, and absent any new symptoms, I’d like to discuss the question of whether cancer can ever be contagious and if so, under what circumstances. Remember that I am not a physician. I use reputable sources (Johns Hopkins, National Institutes of Health, Centers for Disease Control and Prevention, etc. and I share what those sources are with my readers so they can see the original research for themselves.) This morning, I’d like to spend some time in the National Cancer Institute (NCI) which, like the NIH or the CDC, is a government agency.
Is cancer contagious?
The short answer is “In general, no!” You can’t “catch” cancer from sneezing or kissing. But the story does not end there. According to the National Cancer Institute (NCI):
Cancer is not a contagious disease that easily spreads from person to person. The only situation in which cancer can spread from one person to another is in the case of organ or tissue transplantation. A person who receives an organ or tissue from a donor who had cancer in the past may be at increased risk of developing a transplant-related cancer in the future. However, that risk is extremely low—about two cases of cancer per 10,000 organ transplants. Doctors avoid the use of organs or tissue from donors who have a history of cancer.”
So, that’s one way it can spread. But, like life in general, there are all sorts of qualifications and while a sweeping generalization will get you most of the way towards a solution, it doesn’t always provide you with the information you need. The NCI continues:
In some people, cancers may be caused by certain viruses (some types of human papillomavirus, or HPV, for example) and bacteria (such as Helicobacter pylori). While a virus or bacterium can spread from person to person, the cancers they sometimes cause cannot spread from person to person.”
ibid.
That is, the cancer, itself, cannot spread from person-to-person, but the virus or bacteria that have the potential of causing cancer can spread. Here is what that means in practical terms. The human papillomavirus is spread from person-to-person as a sexually-transmitted infection. Women can get the HPV, though it is more prevalent in men. If someone is otherwise healthy:
. . . [their] body’s immune system gets rid of the HPV infection naturally within two years. This is true of both oncogenic and non-oncogenic HPV types. By age 50, at least 4 out of every 5 women will have been infected with HPV at one point in their lives. HPV is also very common in men, and often has no symptoms.
If the viral strain of HPV is cancer-causing (oncogenic) and the person’s immune system is compromised, there is the potential for a different outcome:
When the body’s immune system can’t get rid of an HPV infection with oncogenic HPV types, it can linger over time and turn normal cells into abnormal cells and then cancer. About 10% of women with HPV infection on their cervix will develop long-lasting HPV infections that put them at risk for cervical cancer. Similarly, when high-risk HPV lingers and infects the cells of the vulva, vagina, penis, or anus, it can cause cell changes called precancers. These may eventually develop into cancer if they’re not found and removed in time. These cancers are much less common than cervical cancer. Much less is known about how many people with HPV will develop cancer in these areas.”
Altogether, the HPV can cause six different types of cancer if not treated (and there are vaccines to protect yourself from the HPV in the first place–again, with caveats.) However, there is no cure for the HPV itself while it is in your body, only remediation efforts (for example, treating whatever cancer might arise in that cohort that develops cancer as a result of the HPV.)
To summarize: There is a recommended vaccine (several, actually) to prevent those HPV infection that might someday become cancerous. These specific HPV stains like other HPV strains are sexually transmitted infection. If someone gets HPV, they may in some cases develop cancer before their body can rid itself of the virus. In some cases, a person with a compromised immune system cannot fight the virus successfully.
I don’t want to go any further into human papillomaviruses. This is just one example where cancer “may” be indirectly spread in similar fashion from person-to-person. Here are some other viruses that (1) can spread from person-to-person and (2) eventually become malignant from MD Anderson Cancer Center:
Epstein-Barr virus (EBV) is a herpes virus that’s spread through saliva. EBV infection increases the risk of Burkitt lymphoma, some types of Hodgkin’s and non-Hodgkin’s lymphoma and stomach cancer. There is currently no vaccine for Epstein-Barr virus.
Hepatitis B virus (HBV) is spread through infected blood, semen and other body fluids. Hepatitis B is a leading cause of liver cancer. The hepatitis B vaccine is recommended for all children and adults. If you are not sure if you’ve been vaccinated, talk to your doctor.
Hepatitis C virus (HCV) is spread through infected blood. Hepatitis C is a leading cause of liver cancer, and can cause non-Hodgkin’s lymphoma. There is no vaccine against hepatitis C, but it is highly treatable.
Human immunodeficiency virus (HIV)is spread through infected semen, vaginal fluids, blood and breast milk. While it does not cause cancer directly, researchers believe it increases the risk of cancer by damaging the immune system, which reduces the body’s defenses against other oncoviruses. It can enable other oncoviruses to cause cancer. HIV-associated cancers include Kaposi sarcoma, non-Hodgkin’s and Hodgkin’s lymphoma, cervical cancer, and cancers of the anus, liver, mouth and throat and lung. There is no vaccine against HIV.
Human herpes virus 8 (HHV-8) is related to Kaposi sarcoma in people who have a weakened immune system. That includes patients with HIV.
Human papillomavirus (HPV) has at least 12 strains that can cause cancer in men and women, including anal, cervical, penile, throat, vaginal and vulvar cancer. Boys and girls age 11-12 should get the HPV vaccine. It’s available for patient from age 9-26.
Let’s look at Non-Hodgkins Lymphoma. According to the Mayo Clinic:
Non-Hodgkin’s lymphoma is a type of cancer that begins in your lymphatic system, which is part of the body’s germ-fighting immune system. In non-Hodgkin’s lymphoma, white blood cells called lymphocytes grow abnormally and can form growths (tumors) throughout the body.”
Once again, while there are a number of possible causes, particularly genetics, in some people who have contracted a virus from someone else (e.g. the Epstein-Barr virus that is spread through the exchange of saliva, which then can cause infectious mononucleosis, the “kissing disease” that affects so many teens and college students, and years later “may” cause Hodgkin’s and non-Hodgkin’s lymphoma as well as stomach cancer.) See also here.
As the Mayo Clinic summarizes:
Certain viral and bacterial infections appear to increase the risk of non-Hodgkin’s lymphoma. Viruses linked to this type of cancer include HIV and Epstein-Barr infection. Bacteria linked to non-Hodgkin’s lymphoma include the ulcer-causing Helicobacter pylori.”
The Epstein-Barr virus–which is a form of herpes virus–has infected more than ninety percent of the human race worldwide and has also been indicted for causing Multiple Sclerosis.
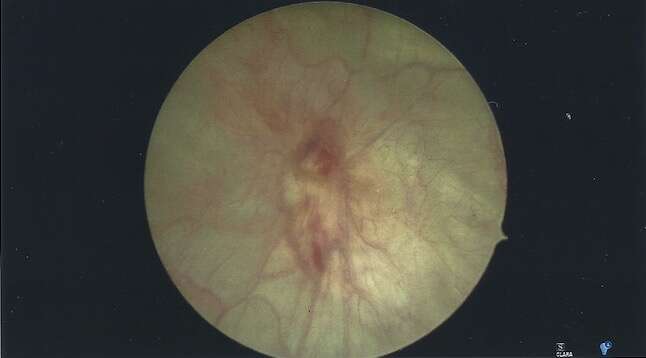
WHAT THE INSIDE OF MY BLADDER LOOKS LIKE
My surgeon passed these photos on to me that she took as she began my second procedure. Before I hang these on our kitchen refrigerator, I thought I’d share them with you.
This photo proports to show areas on my bladder wall where cancer was removed. The red is likely blood in the bladder adhering to the camera lens.
This looks like the canal system on Mars in the old 19th century prints by Lowell and others. The lines are likely blood vessels.
WEDNESDAY, MARCH 1, 2023 (C DAY +30)
It’s 9:00 a.m. and I just showered in preparation to visit my PCP. I had hoped to ask for a repeat of my pulmonary function tests since the last one I had was in 2018. But she recommended I have a CT scan of my lungs. As part of my cancer surgery workup in January, I had a chest x-ray and the radiologist noted in my report that I have a comparison of that x-ray with an older check x-ray. So, I ordered the films from my last hospital/clinic in Texas. What I did not know was that the radiologist in January mentioned in my records that a CT might be useful. Had I note seen my PCP for six months, it would have been that long before I got the scan. So my PCP reordered it today. She also ran a urinalysis and a urine culture to rule out infection. It will likely be Friday before I hear whether there are any colonies of bacteria growing. However, my urine shows that I’m spilling some protein, and there is some urobilogen present above the normal limit as well as 2+ microscopic urine. The urobilogen can suggest liver problems, but my liver functions were checked last month and we normal, so I’m not expecting anything there. Protein in the urine can suggest kidney failure and I do have a reduced filtration rate for me age, but nothing more than the last five years or more nor enough to cause problems in the long run.
“A general rule of thumb is that it takes one week to recover for each day you spend in the hospital. Below are some strategies to help you reduce stress after discharge and get on a clear path to recovery.”
I had a pretty active day. Went to the market, made a few stops besides the doctor’s office. But I was somewhat tired when I got home. Conventional wisdom (which applies particularly to seniors) states that it takes about a week to recover for each day in the hospital.
THURSDAY, MARCH 2, 2023 (C DAY +31)
3:05 a.m. Late last night, I received a note from my pcp saying that the three assays on my urinalysis from yesterday (urobilogen, protein and particularly the microscopic hematuria) were likely elevated as a consequence of my repeated catheterizations and cystoscopies (including the scraping of cancerous and healthy tissue from my inner bladder wall.) My PCP is a truly wonderful doctor (the best PCP I’ve ever had or have worked for.) She also cares for Deena as well. It’s important for a patient to have a personal physician they trust completely, because that doctor can inspire confidence when a patient might otherwise be confused or falsely alarmed. From 1979-1985, I taught in the Nursing Department at the USAF School of Health Care Sciences. I recall that during that time, I read an article in either “JAMA” or the “New England Journal . . .” about the relationship between a doctor’s expressed concern for their patients and their patient’s response to unfavorable outcomes.
Stock photo. Not intended to represent my doctor (or me.) Credit: Daniel Besic (iStock.)
The conclusion of the study said that when a doctor spent a few moments chatting with their patients at the beginning of each visit, asking about their family, making eye contact, etc., the patient was less likely to complain about the doctor or seek legal representation if things went south for the patient (as they sometimes do despite heroic attempts to restore health.) But, those doctors who would their greet patients with questions such as “What is your problem today?” or those who would not make eye contact or spend time with their patients would never develop a mutually beneficial rapport and would usually be rated less favorably over time. It is also wise to rehearse what you plan to say to your doctor before you meet him or her. I try to sum up my problem in less eight seconds or less. If it takes me longer than that, some doctors may accidentally misunderstand me while others either latch on to an unimportant detail or take my complaint in a different direction than I intended. One of the “laws of learning” is “that which is learned first is learned best.” It is very difficult to disabuse a wrong conclusion once someone (including a doctor) misunderstands you or charts the wrong diagnosis or history. Here again, this does not happen with my PCP and for that I am truly appreciative.
FRIDAY, MARCH 3, 2023 (C DAY +32)
Today has been a so-so day. Deena was up with Mollie last night who had some gastrointestinal bug and needed to go outside repeatedly. Today, I went to the store for some groceries before the snow arrives tonight. Around noon, I had a Zoom conference on how to set up my new CPAP, and then I needed to go out again to get some distilled water and windshield washer for the Brono so the hose didn’t freeze and crack in the cold. I was careful not to confuse the two liquids as I added the distilled water to the CPAP.
I wanted to research “tipping points” a bit to explain how my cancer surgeries knocked some of my liver and kidney values temporarily out of whack, but I’m not ready to present the whole enchilada just yet. However, by way of prologue, there are all sorts of tipping points in our l lives. Imagine an old-fashioned balanced scale with two pans. When the pressure on the two pans is equal, the scale is balanced. But add to one side to the exclusion of the other and the scale will shift. When both sides of the scale are equally balanced, you are at a tipping point.
One health-related tipping point might occur in mental illness (euthymia, as when you are normal in mood and affect vs. depression.) Someone with depression who is “balanced” is taking the optimum dose of the preferred drug. That is their tipping point. Diabetics are constantly trying to maintain that equilibrium between sugar and insulin. In either of these three examples, it is possible to go permanently off the scale. Something like an illness or surgery can knock a diabetic out of whack. I did note an interesting point. According to Johnson & Johnson Health & Wellness Solutions who cited a major, recent health study:
The study revealed that the “tipping point” in adult health occurs at age 45.5, after which health starts declining at an accelerated rate. After this point, an “avalanche” of increasing health issues leads to a spike in morbidity and healthcare costs. This study validates an existing model that suggested that once an initial disease state occurs in older adult life, others follow.”
The number 45.5 or five months past your forty-fifth birthday may represent a median age. For some people, it may be lower that that age. In the case of those blessed with good health, it will doubtlessly be a bit higher. This statement suggests that around that age you are probably in your prime, and chronic illnesses are not too far away.
SATURDAY, MARCH 4, 2023 (C DAY +33)
A few inches of fresh snow overnight. I scored a 29 on my first night on CPAP. This is probably an abysmal score, but the machine had all sorts of encouraging superlatives for me. I earned this score essentially by keeping my mask on in the general direction of my nose and remembering to press the power switch on the machine. With no where to go but up, I hope to do better tonight.
I’m feeling okay, but my stamina hasn’t recovered to what it has in the past. I’m looking forward to walking on the track again at the local YMCA.
MONDAY, MARCH 6, 2023 (C DAY +35)
This will be a busy week. This afternoon, our granddaughter comes to visit during her Spring Break. Tomorrow, we have a telemedicine appointment with my surgeon who will go over the second pathology report and likely pass me on to the next doctor for continuing care and surveillance. On Thursday, Deena leaves for Ireland on a visit with her family, and this Saturday our daughter comes to visit until Deena returns plus a few extra days beyond that. That way, I’ll have adult supervision around the clock! No fun in that . . .?
Deena and I understand two important points relating to my cancer to date. The first is that it is an aggressive form of cancer (i.e., “high-grade”) which tends to return, but it has not invaded the muscle liner of the bladder as yet–at least as far as anyone can discern. That makes patients in my circumstance the primary beneficiary of BCG (Bacille Calmette-Guerin) treatment. Except (point #2) that BCG remains in short supply, and the oncology center may not be able to get it locally if at all. It is possible for one clinic to shop around until they find the preparation at another clinic and offer to purchase it on my behalf, but clinicians will tell you that if a clinic has this valuable and scarce commodity, they will likely keep it for their own patients rather than barter it away. So, I may be required to take another therapy, such as chemotherapy instead. If there is a silver lining to this cloud, it is that chemotherapy would not be administered to me through a blood vessel, but rather infused directly into my bladder. In theory, this would spare me some of the ravages of the treatment (hair loss, nausea, etc.)
Drug shortages such as Albuterol needed by asthmatic patients for rescue inhalers, children’s Tylenol , Atorvastatin, as well as shortages in baby formula, feminine hygiene products, etc.) persist causing needless loss of life in some cases even as health care staff scramble to cope. There are a number of reasons why there is a shortage including the costs of manufacturing drugs that provide companies with only marginal profits, globalization where people in Third World countries now have access to these drugs creating even greater demand, corporate bankruptcy, recalls of defective ingredients, problems in the supply chain, the need for FDA approval, even the Russian invasion of Ukraine, and so on. Tomorrow, I’ll share what my surgeon has to say.
The FDA maintains a database of medicines in short supply here.
TUESDAY, MARCH 7, 2023 (C Day +36)
So, my doctor says she’ll start me on chemo because the preferred BCG immunotherapy drug is still in short supply, but then she signed me up for a clinical trial which gives me a 50/50 chance of getting the BCG reserved for trial participants after all or, if not, at least the chemo which I would have received in any event. No placebo in the trial, so I have nothing to lose and everything to gain. Treatment starts in two weeks. My oncologist feels pretty good about my prognosis, though she believes it’s likely that the cancer will return in the future. That being said, they will scope me regularly.
The chemotherapeutic cocktail I will be receiving if I fall in that category of the study is part Gemcitabine, part Docetaxel. The study involves determining whether BCG is more efficacious than Gem/Doce (and vice versa.). This Friday I will process in to the study by completing the necessary disclosure and consent forms and having some blood drawn and tested.
THURSDAY, MARCH 9, 2023 (C Day +38)
Costs on my cancer treatments to date (starting with the CT-scan on the 18th of January) exceed $50K, and our insurance will hopefully cover that (Medicare and Tricare.) I’m not sure about the clinical trials. I meet with the intake representative tomorrow and will go over the financial aspect of the program. After consulting with Medicare and Tricare, it seems like they will cover most costs while the study sponsor pays for some unique costs. These are the areas I need to visit about. I’m starting to wonder how well I’ll tolerate the treatments (the consent agreement for the trial has all sorts of worst case scenarios from me dying from sepsis because someone pokes a hole in my bladder to me being eaten alive by a giant octopus!
Im starting to entertain some concerns about the treatment ahead. One of the two options has a high alcohol content, and the contract warns that patients can become intoxicated from the alcohol being absorbed by their bladder. I’m thinking “alcohol is metabolized by the liver, and I have a sensitive liver (nonalcoholic fatter liver disease.) So I wonder whether my liver enzymes may rise and whether my liver over time might become cirrhotic. It’s times like these that are best left in the hands of a loving Lord.
Dee leaves for Ireland today for a well-deserved R ‘n R visit with the girls in her family. I’m missing her already.
For my Friday post, I hope to share more about the clinical trial. A note from my PCP was encouraging and she said I was a “good fit” because I would play a very small but important role in helping others downstream based on the results gleaned from me.
FRIDAY, MARCH 10, 2023 (C Day +39)
My granddaughter drove me to the clinic this morning to meet the clinical trial coordinator. She mentioned that this trial would be my only chance to receive BCG, and depending on how the computer randomized the participants, I might not get it even then. She also mentioned that around the state and elsewhere, patients with cancer are only getting partial doses of the BCG preparation in order to stretch it out or allow more people access to it. So, I’ll see how it turns out.
I’ll receive six preparations over six weeks (one per week.) It will be infused into my bladder via catheter and after a few hours, allowed to drain. At the end of the six weeks I’ll have another cystoscope.
I had several forms to complete today along with a blood draw and (of course) a urine specimen was required.
The trial is being conducted by the National Cancer Institute, so I don’t anticipate any problems with insurance.
SATURDAY, MARCH 11, 2023 (C Day +40)
My urinalysis from yesterday is in. I’ve had improvement in some areas over the test from a week ago. My urobilogen level is once again normal and I don’t seem to be spilling protein anymore. The presence of microscopic blood seems to be clearing up as well. I do have the suggestion of a few stray cancer cells or at least transitional epithelial cells which were noted, but I don’t have the training to evaluate the significance of this note. I do know that transitional cells are found in the presence of bladder cancer. so I have to assume that there are still some of these little critters running loose in my bladder.
Many people who get bladder cancer actually get it from their urine. In the case of smokers and in the case of people exposed to Agent Orange (presumably what caused my cancer), the carcinogens wind up in the urine, which winds up in the bladder. It’s the prolonged contact between the bladder wall and the cancer-causing chemicals in the urine over time that allow cancer to take hold in a person’s bladder. Developing cancer on-the-spot is not likely, however. More likely is that there is damage to healthy cells which cause them to produce equally unhealthy (malignant) cells.
The rest of my labs from yesterday came back. My hemoglobin has been slowly dropping over the past month. I’m mildly anemic now, most likely from the blood loss over the last thirty days. But my hematocrit (blood volume) is still normal. There may be something else going on, but my primary care physician will likely give this a thought or two as she carefully reviews my chart. I’m happy with my current liver and kidney functions. Altogether, nine values on my CBC (Blood) and CMP (Chemistry) were out of whack, though a few by only a small fraction of one percent. I’ll send a note this weekend to my primary care physician asking her advice. In the back of my mind, however, I sometimes wonder whether some other Agent Orange issue will crop up in the future?
I told the clinical trial coordinator that “I don’t know my bladder anymore,” because it is behaving differently than in the past. But even as Cortez destroyed his ships having reached the New World (See Part 2 of my journal), I am also stranded in a New World with different rules and unfamiliar threats and landmarks and I must familiarize myself with the terrain, the dangers, the safe havens, etc. and navigate forward.
MONDAY, MARCH 13, 2023 (C Day +42)
Today is my brother’s birthday. He’s nine years older than I and has overwhelming health issues that affect his very ability to interact with others, his understanding of where he is and when it is, and so on.
It is 3:30 a.m. I was awakened by night sweats again and the need to void once more (probably five times so far since I went to bed.) We’re on the cusps of a snow storm poised to pass over the next forty-eight hours. The National Weather Service tells us to expect 8-16 inches of wet snow with winds up to 40 mph which means power lines cut, tree branches down, etc.
Event:
Winter Storm Warning
Alert:
WINTER STORM WARNING REMAINS IN EFFECT FROM 8 PM MONDAY TO 8 AM EDT WEDNESDAY… * WHAT…Heavy wet snow expected. Total snow accumulations of 8 to 16 inches. Winds gusting as high as 35 to 45 mph. * WHERE…The Greater Capital District, Mohawk Valley, and portions of the Upper Hudson Valley in eastern New York. * WHEN…From 8 PM Monday to 8 AM EDT Wednesday. * IMPACTS…Travel will be very difficult to impossible. This includes the Tuesday morning and evening commute. The weight of the snow on tree branches may result in power outages. Snowfall rates will reach 1 to 2 inches per hour at times with locally higher rates possible depending on where the heaviest snow bands develop. Strong winds will also result in very low visibility, especially Tuesday into Tuesday night. * ADDITIONAL DETAILS...This will be a long duration and high-impact snow event. Prepare now for this upcoming winter storm. Instructions: If you must travel, keep an extra flashlight, food, and water in your vehicle in case of an emergency.
The storm starts around 8:00 p.m. and gets serious after midnight tonight as the temperature drops. So, for this cancer patient and others, there are storms without as well as within. I thank God that Deena was able to slip away for a week with family to explore Ireland together. I can share her in her healing, enjoyment and wonder vicariously when she returns refreshed. Thank God for small mercies.
TUESDAY, MARCH 14, 2023 (C Day +43)
I wrote my PCP today about my anemia and the mildly abnormal results of much of my complete blood count (CBC) from last Friday and also from several weeks ago. I can only think of one other time in my life where I had this many discordant values. I mentioned to her that I already have five documented Agent Orange issues related to my tour of duty in Vietnam, and I wanted to hint that she might interpret my blood values in the context of some other Agent Orange issue, not that I’d have any more necessarily. I’ll add more when I hear back from her.
FRIDAY, MARCH 17, 2023 (C Day +46)
I received a call yesterday from the clinical trial coordinator. She needed some additional information on me and mentioned they were waiting on one more lab result before they can begin, most likely next week. So, for the moment, I’m on pause.
Deena comes home from Ireland this evening and you can imagine how excited I’ll be to welcome her and hear about her adventure. I’ve been researching and working on a post dealing with Agent Orange and Vietnam War veterans. It was presumably this exposure to Agent Orange (i.e., dioxin) that cause my cancer in the first place. My daughter is here and I’ve been show her around town.
SATURDAY, MARCH 18, 2023 (C Day +47) CODAT
This is a good place to end Part 3 and begin Part 4, as I feel that I’m about to go through a door this week. There are several reasons for this. The first is that my clinical trial is almost certain to begin any day now. Then, there arises the question of how I tolerate the treatments. If I get the bCG, I get the preferred treatment. But if I show very little discomfort after receiving it, then my oncologist will question whether it is working as it should because you want to feel ill after you receive some weakened bacteria or virus into your system. Feeling poorly means your body is developing antibodies to attack the intruder. This is the immune response. If you feel good, then one wonders whether their immune system is working. Secondly, tomorrow I have a CT scan on my lungs. I’m not sure what it might show or how significant whatever it shows might be, but either way, another piece of the puzzle will be in place.
Fortunately, my loving bride has returned to me after a well-earned, well-deserved visit with her family to Ireland. She returns emotionally refreshed and spiritually renewed. Last evening she regaled me with tales of her journey. I was able to participate vicariously. We hope to plan a visit there together next Spring.
A metaphor?
I know someone struggling with a cancer much more serious than mine. I often drive by this person’s house, which was once a beehive of activity during the day. There were smiles, laughter and waves. Even in the evening, the lights would be on throughout the house, creating a warm, inviting, festive feeling. Lately, there is little outdoor activity and there is only a solitary light, if any, within the house at night. I wonder whether this is symbolic? And what when that light goes out?