Last evening while walking the dog, a neighbor caught my attention. He was chatting with another neighbor, a lady whom Deena and I had met last year. He introduced me to her as someone who was recently diagnosed with bladder cancer. After chatting about the weather, the St Patrick Day festivities and such, I asked the woman what sort of cancer she had. She replied “ovarian cancer.” I’m haunted by the look in her eyes and her tone of voice as she spoke those two words. Deena and I live in a neighborhood where people define themselves by the street they live on, or the breed of dog they are seen walking with. Now, and increasingly more so, they have another variable next to their name: “Judy, the lady with bone cancer” or “Fred, who has lung cancer” or “Ron, the retired guy with bladder cancer who lives in that house over there.” Thus begins my post called “My Journey with Cancer (Part 4)”
Photo credit: Simona Pilolla 2 (Shutterstock.)
In the past (before I had cancer), I would not dwell on the issue of who has cancer and who has not. Now, I feel a kinship of sorts with those who are so stricken. It seems there is a phenomenon called “social glue” that develops bonds between people who share a common trauma or pain together, particularly if under stressful conditions. For example, the children of alcoholic parents. Or, in the black community, people who are victims of police brutality. Or, perhaps among cancer patients? There is a sort of shared experience that forms during stress and suffering. A communion. I can sympathize with sadness and outrage when a young, innocent black motorist is killed while in police custody. But can I truly know what the parent is feeling? Who but those who have lost a breast themselves to cancer really know how other breast cancer survivors feel? Put somewhat indelicately:
It is the trauma in our histories that makes us more susceptible to trauma bonding. . . . When two people come together with these things in common, they become both agents of pain and agents of coping for one another. Creating between them a vicious cycle of revictimization that ensures that neither of them advances beyond the pain that binds them together.”
But today I do know a bit about the suffering of cancer patients. No doubt tomorrow I will know more.
MONDAY, MARCH 20, 2023 (C DAY +49)
I was notified that I was randomized to receive Gemcitabine & Docetaxel (chemotherapy) in my clinical trial vis-à-vis BCG. I wondered how they randomized my selection. Did they take the numbers in my date of birth to see if it was a good hand of poker, or did they toss crumpled paper into a trash can (best of five received bCG?) Probably the computer selected me.
On March 30th, a week from Thursday, I will receive my first chemo treatment, followed by a weekly treatment over the next five Thursdays. On Wednesday, May 10th I get my next cystoscopy. I think I’ll practice singing Beethoven‘s “Ode to Joy” in case I’m conscious for this procedure:
Joy, beautiful spark of Divinity,
Daughter of Elysium
We enter, drunk with fire. . .”
What about the efficacy of Gemcitabine & Docetaxel in combating high grade urothelial cancer? Will it work properly? A newly-released (late February) JAMA study (N=312) says “Yes!” Citing a peer-reviewed study, it noted “Those receiving gemcitabine and docetaxel had better recurrence-free survival and a lower rate of induction treatment discontinuation than those receiving BCG.” Deena and I decided that it would be prudent to visit the urology/oncology department at the local Veterans Hospital to see if they (a federal agency) might have supplies of BCG available for vets. But then I’d need to know the BCG is preferable to Gemcitabine & Docetaxel and I don’t know that now as a matter of fact.
I also had the CT scan of my lungs. My lungs were in pretty good shape, but I have quite a bit of calcification of my cardiac arteries, including my aortic arch, my thoracic aorta, right subclavian carotid artery, etc. In layman’s terms, I’m slowly becoming fossilized. Time to see my cardiologist.
TUESDAY, MARCH 21, 2023 (C DAY +50)
I reviewed my CT scan from yesterday, my medical history and the Agent Orange criteria posted by the Veterans Administration (VA) and it seems that I may have a sixth Agent Orange problem. I’ll file this with the VA for their review. Agent Orange, sometimes called (overly-simplified as) Dioxin, was stored and employed in Vietnam, particularly the area I was stationed in, to destroy the jungle canopy so that the U.S. could monitor enemy troop movements and it was also used on crops if those crops were thought to benefit the Viet Cong or North Vietnamese Army. The toxin works in different ways and over time, so it is no surprise that as long as fifty years later veterans are feeling the effects. By next week I should have a blog post on Agent Orange if anyone is interested in reading more about it.
Ho Chi Minh trail (if you can find it.) Environmental warfare took lives as well. Photo credit: Riccardo Calli (Shutterstock.)
I was very reluctant at first to file for disability. The Air Force awarded me 30% when I retired from active duty, but because I returned from Vietnam alive and without any physically intact, I was somewhat ashamed to file for combat related medical problems when so many heroes sacrificed so much for their country. I could dress myself, raise a family and hold a job the past fifty years but many vets could not. Those who survived had greater need than I, I reasoned. Agent Orange, however, taught me that some injuries that are equally life threatening only become obvious many years later, causing all sorts of cell mutations and irreversible harm to body organs and reproductive systems by the time they become obvious. And then there are the “hidden” injuries to a vet’s psyche. Plus, future children of a parent exposed to Agent Orange may have life threatening injuries as well. What sort of weapons of war are able to accomplish that!? My wife Deena whose late husband served the country with distinction in the U.S. Army encouraged me to apply for increased disability and my compensable disabilities tripled in the following eighteen-month period.
Many veterans about my age do not know much about this and others are perhaps as reluctant to apply as I was. Both groups are struggling in many cases. So, I’m hoping that my post on Agent Orange may shed some light for them.
WEDNESDAY, MARCH 22, 2023 (C DAY +51)
QTC, a contractor for the Veterans Administration that helps the VA process claims called yesterday afternoon to tell me that I need a medical exam (x-rays, pulmonary function tests, blood work, etc.) for my cancer claim and others to move forward, but that there are no available appointments on the horizon. When I asked about the local twelve-floor VA regional hospital only five miles away, QTC told me that the hospital was not equipped or able to accomplish this.
It is very possible that my cancer treatments will be over and I’ll be in at least temporary remission before the VA acknowledges I have cancer in the first place.
Later today, I heard from QTC. They said that if I was willing to travel to Rutland, Vermont, I could be seen next Tuesday at 9:15 a.m. Rutland is almost exactly 100 miles from where we live. I jumped on the offer. But if I didn’t have a car, or a loving wife to drive me, or couldn’t get time off from work, or was too sick travel, then there’s no telling when I would be seen.
SATURDAY, MARCH 25, 2023 (C DAY +54)
The last day and the coming few days involve preparation for my VA appointments in Rutland, VT and in Albany. By the end of next week, I will have completed my first chemo treatment and will likely have some comments on how that went.
TUESDAY, MARCH 28, 2023 (C DAY +57)
So, I had my interview with the VA nurse (contractor.) Deena and I had to drive to to Rutland, VT (100 miles each way) and spend the night in a lodge because of the sheer distance from our home and the bad weather encountered in NY state. The VA reimburses at twenty-two cents per mile and we’ll see if they will reimburse for the room, but probably not. The appointment consisted of a weigh-in, plus vital signs, and a twenty-minute interview with a nurse practitioner about my asthma and cancer. No physical exam. No one listened to my lungs. Except for the vital signs which could have been taken tomorrow at my local VA appointments, this could easily have been done via telemedicine, but . . . Once I have my blood drawn tomorrow, plus get my x-ray and pulmonary function tests, the local clinic will forward my results to Rutland and that person will transmit them along with her notes to the VA. In an uncertain number of “weeks to months” we should get a decision on my disability status (we were told.)
My first chemo treatment is less than forty two hours away. I’ll journal how it went this coming Thursday.
Photo credit: Daria Minaeva (Shutterstock.) Photo is not associated with The Lost Kitchen.
Deena and I are planning a number of activities for the months ahead which should be manageable as far as my cancer is concerned. One example of a fun activity involves “The Lost Kitchen” in Freedom, Maine. Episodes of this interesting hotbed of hospitality in the deep woods can be found on Magnolia television networks. The first cookbook is available on Amazon with another one in the works. You cannot just show up for dinner. You must apply for seats which are highly prized by fans of the program. You apply by submitting a postcard each March requesting a seat at one of their events this coming season (late spring, summer and early fall), and the folks at The Lost Kitchen draw cards randomly to decide whom to invite. Deena and I each submitted a postcard (this is our first try.)
WEDNESDAY, MARCH 29, 2023 (C DAY +58)
This is the eve of my first chemotherapy treatment. I feel pretty good, but largely because my loving wife Deena has been such a blessing and support through all of this. I have so many questions about the road ahead because there is so much unfamiliar terrain. What will be my side effects from Gemcitabine? What will be my side effects from Docetaxel? What sort of damage might either of these powerful drugs do to my white cells, red blood cells, platelets? Or, to my liver or kidneys? How effective will these drugs be in preventing the recurrence of my cancer? What is involved with restaging and how many times will I go through it by year’s end? All will be revealed in good time, I suppose.
Deena took me to my three VA appointments today. I received a chest x-ray, a pulmonary function test and had some blood drawn. That should satisfy the VA. Hopefully, we’ll get some positive news from them shortly.
p.s. I hope I don’t come across as pretentious or self-absorbed in all of this. I’ve searched high and low for “first person accounts” of people undergoing similar cancer treatments without and success. Had I found some accounts, I might know better what to expect. Perhaps by journaling my experiences others can benefit?
THURSDAY, MARCH 30, 2023 (C DAY +59)
Well, it’s 2:15 p.m. and I’m half-way through my first chemo treatment. I was in a typical family practice room on a treatment table for two hours lying on my back. The only difficult part was catheterizing me (they promised to use some lidocaine analgesic gel next week.) That was very uncomfortable.
A nurse practitioner computed the dose of Gemcitabine and constituted it in normal saline. I barely felt it go into my bladder. Then, I amused myself on my phone until time to drain it ninety minutes later. At that point she drained as must Gemcitabine as she could and injected the Docetaxel. At that point she removed the catheter and I’m currently at home. The Docetaxel must stay in my bladder for two hours and then I must drain it via urination. It cannot remain in my bladder longer than two hours. No pain so far, though the nurse said it may take several treatments until I feel any pain, sort of a cumulative effect. They do a urinalysis before each weekly treatment looking for blood in my urine. If they find any, they reschedule that day’s treatment. I’ll also have to take sodium bicarbonate in the future before treatments. That seems to be given to shift my pH to the right (i.e., make my body less acidic), perhaps to enhance the potency of the chemo drugs.
Deena was again at my side and I couldn’t have gotten through this without her support.
FRIDAY, MARCH 31, 2023 (C DAY +60)
Slept well and feeling okay today.
SATURDAY, APRIL 1, 2023 (C DAY +61)
My loving wide Deena took me for a day out to my favorite haunts. It was sort of a celebration of what is vis-à-vis what might have been a day or two after a chemotherapy treatment. We drove to Saugerties, NY where we once lived for a year. We went to the Smoke House of the Catskills, a sort of German meat market with German Easter cakes, candies, and so on. From there, we stopped by the Barnwood Restaurant in Cairo for a chicken dinner before coming home. Back in town, we went to a wild bird store to buy a bird feeder and some bird seed. There were three of my favorite places. I never cease to be amazed at how much my wife pampers me. But, I’m certainly not complaining.
In John 10:10 Jesus tells us that he has come that we might have life and more so, abundant life at that. I’ve seen the horror of people ghastly ill from chemotherapy (including my own father) and what radiation does to people’s breast tissue and such over time. I may have to deal with something like this myself someday. But as long as I can, I want to be as humble and appreciative to my Maker for the gift of life. And I want to be appreciative to my family, friends, and most of all to my loving wife!
SUNDAY, APRIL 2, 2023 (C DAY +62)
Palm Sunday: Deena and I went to a neighborhood Espicopalian church today. They passed out palm fronds and had everyone march around the sanctuary several times. I suppose it was an attempt to recreate the excitement in Jerusalem two thousand years ago. I managed to stumble over the edge of a platform, the height of which I badly misjudged. Fortunately, I was able to catch myself. After ten minutes, four children and thirty seniors over sixty-five made their way slowly back to their pew. That was my exercise for the week. The people were nice and generally welcoming. I liked the pastor, but, in the words of Bono and U2, we “still haven’t found what [we’re] looking for.” Dee and I discussed visiting St. Peter’s Episcopalian Church in the capital where Lt Colonel George Monro from Cooper’s “Last of the Mohicans” book is buried. No, he wasn’t killed on the way to Fort Edwards by Magua in August 1757. He died in Albany of a stroke in November of that year.
Cancer grading
I wanted to discuss cancer grading. The grade of a person’s cancer is in many ways as important as the stage that it’s in. We all know that a Stage III cancer is something very grave. But what about grade?
In most cases, doctors need to study a sample of tissue from the tumor to decide if it is cancer and, if it is, its grade. They obtain this tissue by doing a biopsy, a procedure in which they remove all or part of the tumor. A specialist called a pathologist determines the grade of your tumor by studying samples from the biopsy under a microscope. The pathologist describes the findings in a pathology report, which also contains other details about your diagnosis.
Cells that look more normal might be called well-differentiated in the pathology report. And cells that look less normal might be called poorly differentiated or undifferentiated. Based on these and other features of how cells look under the microscope, the pathologist will assign a number to describe the grade.”
Some cancers have their own grading systems but most solid tumor cancers are given a grade between 1 to 3 or 4. (Solid tumour cancers, like breast or prostate cancer, form lumps.) A lower number means the cancer is a lower grade. Different parts of a tumor can have cancer cells with different grades. But the tumor is usually graded as the highest grade seen anywhere within the tumor.”
So, a tumor can have mixed cells, where most might low grade cancer cells and a few other cells high grade cancer cells. But the presence of even a high grade cancer cells will automatically give the tumor a high grade classification.
The grading of blood cancers is a bit more complicated.
If you want to find out detailed and easy-to-understnd information on another type of cancer, see this excellent website run by the National Cancer Institute.
WEDNESDAY, APRIL 5, 2023 (C DAY +65)
Tomorrow, I have my second chemotherapy treatment. This time, it’s at 2:00 p.m. so things will have to move along fairly smoothly if I am to be released before the clinic closes. I read that 51% of patients have at least one bad reaction to the two medications I am receiving during my six-dose course. That’s not to say that I will, however.
I’ve been considering what my cancer and cancer treatments mean over the short and long term. For a number of years, I’ve been juggling several chronic health issues. For example, I’ve been flirting with chronic kidney disease (CKD.) I have some benign cysts in my kidneys that are not growing, but the presence of the cysts means that much less functioning kidney tissue. Fifty years of taking medicine for migraines or elevated blood pressure has a cumulative effect as well. So, I’m sometimes in Stage III of CKD, but more recently Stage II (of V stages.) Then, there is my COPD that was noted on my January chest x-rays for the first time, but not on my CT-scan three weeks ago (though I’m not sure the CT would pick it up.) I also have some heart issues (issues with my aortic valve and moderate global calcification of the arteries in my heart and elsewhere in my chest. This is an irreversible process, even though my cholesterol is generally normal.) Then, there are some mental health issues such as occasional depression, stress, mild anxiety and insomnia (which is why I’m writing this at 3:30 a.m. instead of sleeping.) These symptoms are likely associated with PTSD and possibly my Parkinson’s Disease, though most normal people are not strangers to these problems. I don’t dwell on these concerns, but they do pop up in my mind if I fall, get a troubling value on a liver function panel, or an abnormal chest x-ray.
Chronic diseases are like a pack of hungry wolves. The disorders predictably flare up when the patient is weakened or body systems distracted by some emerging and more demanding health crisis. To me, it suggests the behavior of a wolf pack, as described in this account:
Wolves strike their prey at angles and try to separate weak members from the group and take turns nipping at their prey until it is exhausted and vulnerable. . . Wolves usually attack from behind and the sides, with experienced wolves usually taking the lead, feinting and attacking from opposite sides until a crippling bite or slash can be made to leg muscles that slows and brings the prey down for a killing or incapacitating bite to the throat.”
The analogy of wolves is not quite apt, of course. Wolves work as a team to bring down their prey. The loss of one wolf does not deter the pack from the hunt. Body systems, however are linked together. Pump failure of the heart means less blood to the kidneys. Sepsis (infection) in one part of the body (such as the appendix or spleen) can cause shock or the death of the patient. Nor are future health problems limited to what you already have at any given moment. Something worrisome can appear out of nowhere. But your chronic issues do not get better, only worse over time. There is no cure for Alzheimer’s, arthritis, MS or Parkinson’s Disease.
In medicine, there are what are called “opportunistic infections.” Opportunistic infections can be described as “. . .infections that occur more often or are more severe in people with weakened immune systems than in people with healthy immune systems.” Examples can be found among bacteria, parasites, fungi, viruses and yeasts. For example, oral thrush might emerge if a patient is seriously ill with some other health issue, perhaps shingles. But something like thrush does not appear out of nowhere. It is present on a sub clinical basis or at least environmentally available. Or, a person with a serious burn across forty percent of their body might develop tuberculosis, which otherwise would be inactive, neatly sealed in a spore and forgotten elsewhere in their body. AIDS patients can develop Kaposi’s sarcoma, another opportunistic disease, though the most common opportunistic infections are probably staph and strep illnesses, issues affecting the biome of the gut, etc.
Opportunistic infections can be life threatening:
Opportunistic infections are a major cause of illness and death in oncology patients and are the leading cause of death in recipients of renal transplants.”
Then, there are just plain complications. Some drugs needed to treat certain cancers can cause congestive heart failure. Statins, oral contraceptives, even some antibiotics can damage a person’s liver beyond repair. You can’t live without your liver, and a bad liver causes brain damage. A diabetic who has stable glucose levels will find that a COVID infection (or even a common cold) may cause his glucose levels to soar. You see evidence of the potential for complications every time a commercial for a medication is advertised on television. One drug may cause suicidal tendencies, another the potential for a stoke. Even over the counter drugs like Tylenol(TM) can cause life-threatening issues if taken in large doses or by people who may be sensitive to acetaminophen. But these instances are fortunately rare. There are approximately 72 million women on birth control pills at any given time, and they are not all in liver failure, yet alone .005 of one percent of them. Perhaps not a single one of them are, but the medication has the potential of harming a patient who might be vulnerable.
Thankfully, I have a gracious God and a loving wife who both watch over and care for me around the clock. Deena has never envisioned herself as a caregiver, but she is doing just fine. I like to remind her what the British slave-trader-turned-clergyman John Newton once said: “God saves dying grace for a dying hour.” In other words, there may come a time in your life when you need to lift a collapsed car off some poor soul injured in an automobile accident. At that moment, you may find yourself imbued with superhuman strength, though don’t expect to depend on it at times you don’t actually need it.
More tomorrow after my treatment.
THURSDAY, APRIL 6, 2023 (C DAY +66)
9:42 a.m. Four more hours to go before my second chemotherapy treatment. I’m starting to understand that positive thinking and a good attitude does not completely vanquish what is happening. Like cleaning an area of a carpet of a dark stain, sometimes a faint remnant of the stain remains and if you know where to look, you can see it even if others cannot. And with the stain comes the reminder of the event that caused it. So, too, while even though this morning I am laid back and while I can banter light-heartedly with Deena over something amusing that someone sent to her Facebook account, subconsciously I am aware of the treatment ahead, and so I was last night as well.
I think part of the problem may be a loss of contol over some part(s) of my body. I’ve had almost three quarters of a century of knowing “me” inside and out, and now I’m having to re-learn certain fundamental things (like how long I have to get to the bathroom.) I know that it is difficult enough if there is a slow, gradual decline as many people have in terms of memory, mobility, etc. But it is more disconcerting if the loss is abrupt.
5:50 p.m. Treatment is over. I feel a bit dehydrated since I’ve been NPO (nothing passed orally) since this morning. So far, so good, thank God!
MONDAY, APRIL 10, 2023 (C DAY +70)
Deena and I spent Easter Sunday with family up here. No issues yet from my chemotherapy and therefore no prescribed restrictions or physical limitations on my activities. We won’t get an idea on the state of my cancer until Wednesday, May 10th when my oncologist scopes me again. It’s possible she may take a biopsy or two. Soon after, I’ll be re-staged if there are any noticable changes. We’re also waiting for the VA to acknowledge my cancer, since it is presumed according to VA criteria to be caused by Agent Orange exposure from my tour of duty in Vietnam.
I’ve been working on other blog posts given the current state of world affairs. If you click on the “Home” menu option near the top of your screen, you can seen the 140 or so posts that are available on health, travel, science, history, politics, religion and so on. I’m also trying to organize the blog posts on cancer into some meaningful framework.
I apologize if there are not cancer-related posts every day. Hopefully, I won’t have a lot to write about in the near future. But high grade bladder cancer seems to be something difficult to shake, so I’m sure that over the long term, I’ll have much more to report about my saga. In the meantime, Deena and I are planning an active future, God permitting. In the words of poet Robert Frost who reposes only an hour or two from where we live:
“The woods are lovely, dark and deep. But I have promises to keep, And miles to go before I sleep, And miles to go before I sleep.”
Bennington, VT, USA October 15, Leaves fall on poet Robert Frost’s grave in Bennington, Vermont.Photo credit: James Kirkikis (Shutterstock.) Editorial use only.
WEDNESDAY, APRIL 12, 2023 (C DAY +72)
I think I’m having a bit of depression. It’s partly a mood disorder, but also the perception that the simplest tasks are getting much harder to accomplish than normal. Like typing accurately. It’s also the notion that I’m threading water (neither sinking nor swimming.) Meanwhile, I feel a bit washed out, listless.
The VA wants me to have another in-person evaluation on my hearing to document any hearing loss (less than a year after they tested me for hearing aids and which I’ve had since last summer.) In fact, I’ve had my hearing tested each year for three years and each time it’s worse. They have these three hearing exam results but I suppose want a fourth one for some reason. They also want to check for tinnitus (ringing in my ears), and they want to evaluate a scar that I don’t even have (it is inaccurately classified in their records.) Deena may have to drive me fifty miles one way (or more) only to have the examiner refuse to look at the scar, unless their script says “Look at scar.” Some examiners are eagerly engaged and genuinely interested in the person they are interviewing and they go the extra mile. Other examiners appear to wish they were fishing or were somewhere else. When I was interviewed about my cancer, the VA contract examiner didn’t want to see the surgical reports, the pathology reports, the CT-results, etc. which I had painstakingly assembled and brought with me. They just asked me if I had ever smoked, or when did I first notice blood in my urine, questions like that..
Yesterday, I got a notice from the VA scheduling contractor that my urinalysis and chest x-rays from two weeks ago were significantly abnormal and required immediate attention. They gave me a number to call if I wanted to get a copy of the results to share with my doctor. I called and they sent me a form. The form was a Freedom of Information Act request. An FOIA! To get the results of my urine test?! And in a hurry?! If it wasn’t so funny, it would be sad.
“If you are a vet who fought in Vietnam, you’re probably at risk for bladder cancer. You should ask your family doctor to run a urinalysis on you to check for hidden bleeding.”
Next month is Memorial Day, an opportunity for our elected leaders to proudly wave miniature American flags, give patriotic speeches and have their photos taken at veterans cemeteries with grim faces and tears in their eyes, lauding the sacrifices vets have made in service to the country long, long ago and far, far away. Then, like with Veteran’s Day, it’s off to some other venue. Another speech, another call to a wealthy donor for support, another scotch? The same goes for Veterans Day. Vet’s don’t need congratulatory speeches and plastic poppies to wear once or twice a year. They need our representatives to understand that for vets, the battle goes on. We lost the war in Vietnam, but Vietnam vets are still dying from combat-related causes. Why not public service announcements on billboards and television saying: “If you are a vet who fought in Vietnam, you’re probably at risk for bladder cancer? You should ask your family doctor to run a urinalysis on you to check for hidden bleeding.” The irony is, it wasn’t the Viet Cong who poisoned our troops with Agent Orange. We did it to ourselves!
Words. Photo credit: Bill Perry (Shutterstock.). Editorial use only.
Perhaps it is this sort of frustration in extreme that led nineteen vets to commit suicide in the parking lots and elsewhere on the campuses of VA hospitals in one year back in 2017-2018? Fortunately for me, I have a loving, supportive wife, a family, and the ego resources and motivation to press on.
Tomorrow this time, I’ll be halfway through with the first regimen of chemotherapy. I’ve been researching why some patients develop low grade cancer and others develop high grade cancer (the more serious of the two.) While the literature I’ve seen so far is only circumstantial at best, it seems that one reason people develop high grade cancer may be because of the nature of the carcinogenic agent itself.
THURSDAY, APRIL 13, 2023 (C DAY +73)
11:00 a.m. Just arrived home. I still have the Docetaxel inside of me and must not void before 12:45 p.m. Procedure went okay. So far, so good.
Last night around bedtime, our septic system backed up and overflowed in our basement. Deena called our plumbers and they are working on the system at the moment. Unfortunately, she was not able to get much sleep last night between planning for today’s chemo appointment and the unexpected crisis.
My spirits have improved after Deena and I went out for dinner, talked everything through and shared some prayer yesterday evening. It also helped for me to work on some assorted blog posts. As far as the VA is concerned, I think it best to just let my status quo (i.e., getting the VA to acknowledge my cancer and Parkinsonism as service-connected through Agent Orange exposure) simmer on the back burner for the time being without obsessing over it. I’ve been reminded of a Bible verse in John 12:24 where Jesus says:
Very truly I tell you, unless a kernel of wheat falls to the ground and dies, it remains only a single seed. But if it dies, it produces many seeds.”
Hope still lives. Photo credit: Pavlo Baliukh (iStock.)
Jesus is referring to the apparent lifelessness (which we refer to as dormancy) that a seed undergoes when it is separated from the nourishment of its parent, and before it can produce roots in order to rejuvenate on its own. In some cases, this dormancy can last for centuries. This is a natural process which people sometimes refer to as “letting go” when it applies to human affairs. Sometimes we find ourselves in very difficult situations, squeezed between a rock and a hard place. These situations may be relationships, finances, difficulties at work, serious illness in the family, and so on. We have goals and dreams that seem perpetually our of our reach. A situation could be a problem a young aspiring wife has with miscarriages, someone with health issues forced to work beyond their planned retirement age, or a young adult who must defer their dreams. Recall the classical movie “It’s a Wonderful Life” with Jimmy Stewart who, as the eldest son, must tend to the family business instead of leaving home and carving out a life of his own. What we have to often do is to “die” to what we want so we can live when something better comes along. How many failed personal decisions, career choices and financial obligations have happened because someone could not wait patiently for just the right circumstance.
Amber waves of grain. Photo credit: Nasty (iStock.)
When we release the control that a difficult situation imposes on us, the problem no longer has any power over us. Put it aside and ask God to deal with it in His own way and time. Often, though perhaps not always, a resolution to the problem or reconciliation to the relationship emerges when we least expect it.
In the meantime, I’m filing this under “W” for “whatever.”
SUNDAY, APRIL 16, 2023 (C DAY +76)
Sunday. No issues from last Thursday. Now that I’m past the half way mark of the first regimen of treatment, the next cystoscopy (May 10) is starting to loom ahead, sort of like a mountain range as you approach it from the flatlands. It slowly but surely grows in size which means it is increasingly hard to ignore or evade.
There are three possibilities as far as I understand my oncologist. The first is to get a good report after she scopes me and then return to the clinic as some future date (sort of the same type of “watchful waiting” that breast cancer patients have.) The second would be where some traces of cancer are noted and the six week of chemo might be extended. The third possibility would be a recommendation to have surgery to remove the bladder, the prostate, and convert three inches of small intestines into a bladder. Typical hospital stay is a week to two weeks. This is considered to be major surgery with the chance of complication (mainly blood clots or infection.)
I expect to post more in the following days as Deena and I prepare for what may be a decisionmaking process in the weeks ahead.
Knowledge is power
Whenever I faced a hurtle in my life, such as applying for a career change, getting involved in a major project, investing in an opportunity, or confronting a disease or disorder, I always tried to learn as much as I could about what I was facing. I never wanted to make important decisions based on incomplete information. You want to know the best case scenario, the worst case scenario, the most likely scenario and so on. You should also ask what will happen if you do nothing. Sometimes standing pat (firm) is a good choice, even with cancer. And believe it or not, some doctors might recommend taking no action against a slow growing cancer like prostate cancer if you are a septuagenarian or other things in your life are true or present. You also want to know what option your doctor thinks best, because your doctor has an expert opinion. And I check my doctors out before I see them as well. Usually, I look them up with the state medical board, or I consult with my primary care physician. I rarely see a physician unless I know what school they graduated from, where they did their residency, what their specialty is, where they have admission privileges, how long they’ve practiced, what disciplinary action–if any–has been taken against them, and so on.
When you feel overwhelmed by cancer
Hand of a man drowning in the sea trying to float. Photo credit (Thinkstock.)
There’s a certain paralysis that occurs when you feel overwhelmed. When I was a nursing ward supervisor in the Air Force, I was called in one night because of an after hours issue on the ward. After I arrived, the on-duty technician was literally running in circles. I asked him what the problem was. He said the Emergency Room just admitted three patients to the unit, and he didn’t know where to start. I asked himcabout the status of the patients. One patient, I was told, was to be prepped for surgery for an appendectomy in the next few hours. The second patient had a diagnosis of “R/O M/I” or rule out a myocardial infarction (heart attack.) I quickly asked about the third patient. The technician said “He lost his leg.” I asked how and the technician replied: “I don’t know–it happened twenty years ago!” So, I had to ask why he was on the unit at the moment. Apparently, he had a kidney stone or something like that. But this technician had to admit all three patients and he was thoroughly overwhelmed because he could not prioritize who to do first. I told him he should prep the pre-op patient for surgery and I would work with the patient who was having chest pains. The patient with the kidney stones could wait. Fortunately, all three patients survived. This is one way to deal with being overwhelmed–ranking or prioritizing your issues or variables.
So, when dealing with cancer, it should not be any surprize that ranking your treatment options and priortizing goals falls near the top of the list. You should ask yourself what goals can be met if you have a diagnosis of cancer. Some cancers can be treated easily than others. Is this a good time to father a child you there is a chance you may not see the child start school? Should you retire now, assume a mortgage on a home, and so on. In my circumstances and assuming I may need surgery at some point in the future, would it be better for me to have the surgery at 75 than at 80? And should I sacrifice several years of quality life by expediting the surgery? For each of the options, it might help to make a list of the pros and cons of each option.
Communication
I’ve met patients that don’t want to know how they are doing. They would rather their doctor paint a rosy picture of their health. Personally, I’d rather have the truth, but people are different and their wishes should be respected. Most people with a terminal illness (i.e., six months or less to live) have unfinished business in this life and whenever it is that I reach that point, I would likely be no exception. Unlike some patients, I would not hide my diagnosis and prognosis from my family, because they may have unfinished business with me. And certainly, you would not want to hide how you’re doing from your spouse.
Be flexible and prepare for ups and downs
When a person is advanced in years, when they have a number of serious health issues, there are all sorts of disappointments as well as things to be thankful for. At the moment, I cannot receive the best phamacological preparation available for bladder cancer because it is in short supply. Imagine having hypertension, but you cannot get medicine to keep your blood pressure under control. Try not to get rattled, angry, depressed and so on or, if you do, seek counseling, medication or advice if you do. These are all normal emotions.
Use all available resources
There are all sorts of resources available for cancer patients. If I ever need surgery for any reason, and I’d have trouble ambulating or with personal hygeine after hospital discharge, I would apply for a stay at a skilled nursing facility. This is like a “halfway house” medically speaking. Your doctor needs to write the order for this, so you may need to speak to him about your circumstances since it is not alway automatic. You’ll also need to visit with the social worker in the hospital to arrange it.
There is also Home Health, online and in-person resources such as webinars, discussion groups, psychological counseling and spiritual counseling as well.
Plan for what comes next
When your time comes to leave this reality and pass through the veil into the next, you’re actually taking a journey of sorts. Are you prepared to embark? The ancient Egyptians believed they would need “stuff” so the Pharoahs were buried with boats, weapons, wealth, food and so on. Native Americans also gave considerable thought to the afterlife. What about you? Are you ready to meet your Creator?
TUESDAY, APRIL 18, 2023 (C DAY +78)
I’m not sure if I mentioned this before, but bladder cancer is the most expensive cancer to treat of all the cancers we know of. Even back thirty or more years ago this was true. For example, going back to 1984-1990, Medical Care journal noted:
Total Medicare payments from diagnosis to death were highest for persons with bladder cancer ($57,629) and lowest for those with lung cancer ($29,184). Low payments for persons with lung cancer corresponded to brief survival times.”
Those figures are in 1990 dollars. I’ve exceeded that lifetime figure of $57,629 in cancer care and I was only diagnosed ninety days ago. Lung cancer patients tended to die back then as rapidly as many patients with pancreatic cancer die today (the average life expectancy of pancreatic patients after diagnosis is 3-3 1/2 years.) Mesothelioma is even a bit less than 3-3 1/2 years and brain cancer just a bit longer than pancreatic cancer. This is because many patients (at least in the case of pancreatic cancer) are fairly symptom free until they are in some advanced stage of the disease, which makes a cure much harder to achieve. So the costs of care are much more in bladder cancer patients, where some patients can survive many years after first being diagnosed.
The Journal of the American Medical Association (JAMA) Network suggests that preventive bladder cancer screening is not necessarily a priority because what you don’t know won’t cost you any money. See here for example:
The findings of the present study revealed that, despite guideline recommendations, frequent surveillance testing was common and was associated with increases in the annual cost of care over time. These data suggest a need for ongoing efforts to limit overuse of treatment and surveillance, which may in turn mitigate associated increases in the costs of care.”
The word needs to get out to men and women between the ages of 70-80 to request annual urinalysis from their doctors, and if hematuria (blood in the urine) is used to diagnosis a urinary tract infection, then these patients should be retested to see if they might have bladder cancer. Budgetary pressures on doctors may mean that doctors do not encourage patients to be tested, so patients may have to be assertive on their own to be tested.
I wish I had been.
Postscript on bladder cancer grading
According to the National Institute of Health, “Seventy percent of all bladder cancer is low-grade cancer. Ten to fifteen percent of low-grade [cancer] progress to high grade [cancer] at some point.” The exact reason or mechanism for this transition is not known, though some researchers believe that is caused by addition mutations in the cells. Also, it seems like certain carcinogens cause high grade rather than low grade cancers. Again, high grade cancer is more likely to reoccur and spread to other organs.
WEDNESDAY, APRIL 19, 2023 (C DAY +79)
I wanted to go a bit deeper explaining how bladder cancer begins. There are quite technical explanations in the literature, but I will simplfy it as much as possible so it will be easy for each of us to understand. Anything deadly that is absorbed by your body and blood stream whether chemical additives in cigarette smoke, pollutants in drinking water, radioactive substances from industrial accidents or medical testing, street drugs, etc. eventually passes through your bladder. As noted by authors Kalyan Saginala, Adam Barsouk, et al. “The urothelial cells lining the bladder and urinary tract are constantly exposed to environmental, potentially mutagenic agents that are filtered into the urine by the kidneys.” Mutagenic agents are those substances capable of causing potentially cancerous mutations in normal cells.
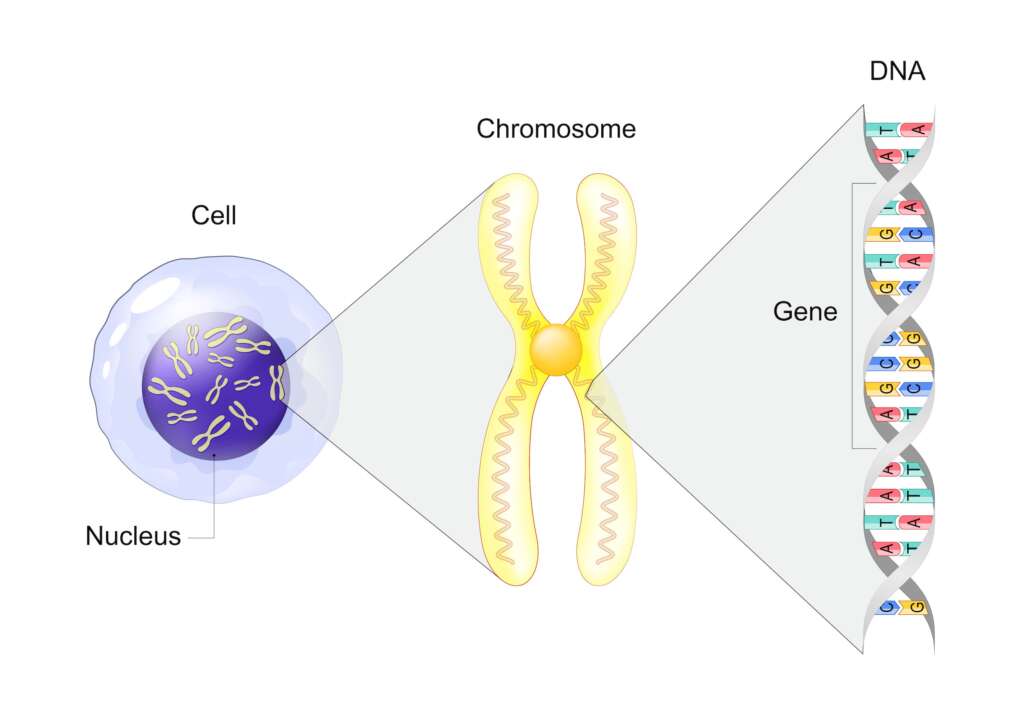
Genes, proteins and cells
There are 50-120 trillion cells in the human body, and the cells, themselves, are microscopic. In spite of this, there is roughly six feet of DNA in each cell. Recall that DNA is represented by a helix found in each of the forty six chromosomes present in the human cell (see illustration.) If you were to carefully unwind all the DNA from the chromosomes in a single microscopic cell, it would stretch two meters (six feet) in length.
So, it should be no surprise that there is enough DNA in each cell for each of the thousands of genes which are also microscopic to populate. Humans have an estimated 46, 831 genes that associate themselves with specific chromosomes within the cells. Pattern baldness, for example, comes from one or more genes on the “x” chromosome, which means it comes from your mother. If you inherited it from your father, it would be on the “y” chromosome. Genes are sort of scraps or sections of DNA. The estimated number of genes we have has crept up over the past few decades since they were first mapped because the definition of a gene has broadened over time as we learn more about them.
Genes have all sorts of designations involving numbers and letters which make sense only to doctors and researchers. In humans, there is a gene called “tp 53” and a protein called “p53.” Proteins are complex molecules made up of amino acids. But we won’t go into amino acids for now.
p53 (blue) tagged with ubiquitin (yellow); p53 prevents cancer formation and acts as a guardian of the genome. Mutations in the p53 gene contribute to about half of the cases of human cancer. Credit: Selvanegra (iStock.)
This tp53 gene is located on the 17th chromosome in each of the trillions of cells in your body. The tp53 gene provides the body with instructions on how to produce a specific protein called tumor protein p53 (see reconstruction left.) Proteins are important in manufacturing new cells and repairing damaged cells. So, this p53 protein is important whenever cells in your body are damaged from radiation, toxic chemicals, Agent Orange and other carcinogens. The purpose of this p53 protein is to protect people and animals from developing cancer, but when people do develop cancer, researchers find that the p53 protein is often mutated or changed in some important, unnatural way itself (mutations in the tp53 gene are the most common genetic changes found in human cancer, occurring in about half of all cancers. Research suggests that chemotherapy is more effective treating those cancers that arise out of mutations in the tp53 gene, at least as far as bladder cancers are concerned.) As a rule of thumb, “the more defective the mutation [in the tp53 gene], the greater the risk” of developing cancer. In fact, “rare inherited mutations in the body’s master regulator of the DNA repair system – the tp53 gene – can leave people at a higher risk of developing multiple types of cancer over the course of their lives.” Mutations mean that the gene can no longer perform its function to ward off cancer because the gene has had its original programming scrambled. Thus, “DNA damage can accumulate in cells. Such cells may continue to divide in an uncontrolled way, leading to tumor growth which can lead to malignant cancers.”
When cells become damaged, protein p53 “activates other genes to fix the damage. If the DNA cannot be repaired, this protein prevents the cell from dividing and signals it to undergo apoptosis.” Apoptosis refers to the death of the damaged cell. “By stopping cells with mutated or damaged DNA from dividing, normal p53 proteins are designed to help prevent the development of tumors. Because p53 is essential for regulating DNA repair and cell division, it has been nicknamed the “guardian of the genome.”
Nuts and bolts
Here are some isolated facts that have no explanation at this point:
Photo credit: WestLight
While Greece has the highest rate of bladder cancer among men in the world, Lebanon has the highest rate among women. I have no idea why this is so. The shortest distance between Greece and Lebanon is 859 miles, yet Greece has the highest bladder cancer rate among men and Lebanon has the highest bladder cancer rate among women. Both are modern countries. Because smoking is the most common cause of bladder cancer, you might think that a lot of men in Greece smoke, but certainly not a lot of women smoke in a country that is becoming more and more Muslim.
Treatment went well today. My cystoscopy has been moved to late June because it was scheduled a month earlier than protocol by mistake. Not a true disappointment for me. You can’t live hoping for good news or dreading bad news. You have to be able to roll with the punches when dealing with something like this. Of course, I’ve lived a better part of a century, so some might say this is easy for me to accept this. Certainly it would be much harder were I a good deal younger with a long life ahead of me. But, “our arms are too short to box with God” as they used to say so you play the hand of cards that you’re dealt with. What else can you do? Both Deena and I have had long happy marriages before our spouses died, so our time together is sort “icing on the cake” in a way. But certainly we both hope and pray for more time together, places to see, miles to go.
Deena and I discussed the possibility of starting a small discussion group of folks with cancer, specifically a men’s group. This would meet every week or every other week at a certain time for lunch and a chance for each of us to get to know others who are laboring under the same condition as we are. A support group I suppose. There is only one other group in the county as far as I know, and that group has not met since the pandemic began, so we’d be starting from scratch. We’ll see how it goes.
Now that we have extra time in May, we’ve booked a flight to Texas for a part of a week to attend a high school graduation (grandson will be stating at Texas A&M in the fall with a major in Vet Medicine.) We’ll also be able visit other family members and some friends before being getting fried by the heat.
Here (below) is another “nuts and bolts” factoid: What do bladder cancer patients die from (if not cancer?)
What are the leading causes of death of patients with bladder cancer by years since first diagnosis?
Bladder cancer survivor (years)
Leading cause of death among patients
Secondary cause of death among patients
Tertiary cause of death among patients
5-10 years
Cardiac disease (11%)
Pulmonary disease/COPD (7.7%)
Bladder cancer (6.9%)
> 10 years
Cardiac disease (8.6%)
Pulmonary disease/COPD (5.8%)
Bladder cancer (3.1%)
“Causes of death in long-term bladder cancer survivors: A population-based study” Jianqiu Kong, Xiayao Diao, et al.
SATURDAY, APRIL 22, 2023 (C DAY +82)
Did some research on the BCG treatment. Thursday night I felt flushed but was afebrile. Yesterday I felt a bit rundown. There may be some sort of cumulative effect over time from the treatments, or it may be something else entirely.
MONDAY, APRIL 24, 2023 (C DAY +84)
I had two VA C&P (compensation and pension) exams. The first was with a very nice Physician’s Assistant (PA) who had quite a few questions about my surgical scar revision and hernia repair surgery which was done just before last Christmas. The information the VA provided her was not only wrong, it was nonsensical. This PA said she lives in Vermont and has to drive to work in NY to meet patients like me, who only two weeks ago had to drive to Vermont to meet someone like her. But hopefully when the VA receives her report the errors will be corrected.
The second appointment was for a hearing test. This was the third hearing test the VA has had me take in less than two years. The VA says I clearly have hearing loss (as my wife would attest) and they have provided me with pricey hearing aids which I appreciate, but they say that my hearing is not in any way disabling to me. I believe my hearing loss was caused partly by working on the flight line while in the Air Force as jet turbine engines constantly whined and partly from the countless rocket and mortar attacks while I was in Vietnam. I had to rule out riotious living, mindless inebriation and other forms of villiany as possible causes of my hearing loss. Not sure how convincing I was. We’ll see how that turned out on some occasion in the near or distant future.
TUESDAY, APRIL 25, 2023 (C DAY +85)
I found an interesting seventeen second video on how a cancerous tumor is removed from a bladder wall during cystoscopy while performing a TURBT.
Here’s another example of shearing off cancerous tissue from someone’s bladder. Note that there is a good degree of magnification to this video. Not for the faint-hearted to watch.Credit: OlympusMedUS.
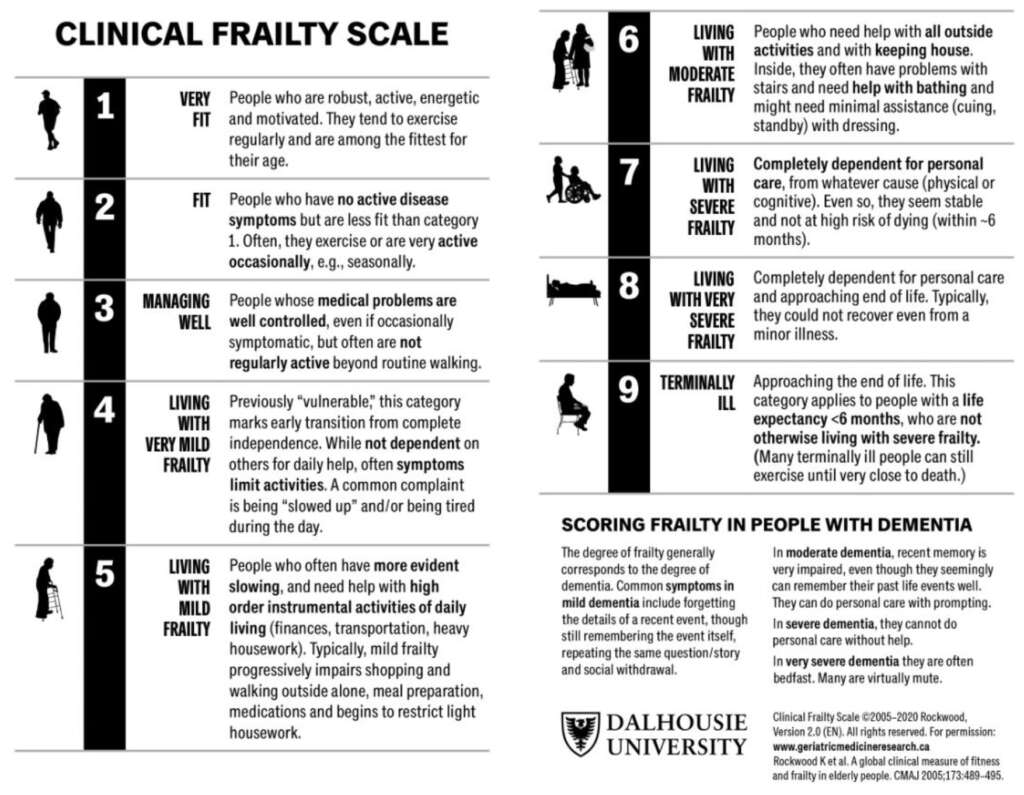
Something else that I discovered that I thought was interesting. When people (particularly seniors) are facing major surgery, part of the surgeon’s decision on how and whether to proceed is based on what is known as a “Clinical Frailty Index.” There are several versions in use, but they are pretty much the same as this one:
Copyright Dalhousie University: Permission granted for non-commercial, educational fair use.
The term “terminally ill” (Category 9 in the chart) is widely understood to mean that a person cannot be cured of a disease and has less than six months to live. However, I do know of people classified as terminally ill who have lived for several additional years beyond the six months. At the point that a person is considered terminally ill, they are often (but certainly not always) either in a palliative care program or a hospice program. So, they may at that point find themselves disqualified for some life sustaining procedure or another. It’s a common misperception that a patient can get any surgery they want (for example, a liver transplant) if they need one and have the money or insurance to cover the costs. However, hospitals have a board that convenes to decide whether a patient should have the transplant, irrespective of what their wishes are and whether they can pay. This is because organs are in short supply and involve a lot of work to perform the procedure. An alcoholic who drinks regularly will almost certainly not receive a liver, nor will a patient who smokes, uses street drugs or perhaps has a psychiatric illness. They must also comply with the follow-up care.
I know of a patient who was an ex-smoker who waited for several years to get a new heart. Then, he got the call. But after rushing to the hospital and getting prepped for surgery, the transplant fell through. The poor guy was so stressed he smoked a cigarette to calm his nerves. Just one. A day or so later, another heart arrived, and as they completed his pre-op blood work, they noted the presence of nicotene or cotinine in his blood. He was then disqualified from receiving the heart.
I apologize for “hopping about” with the items I post. It is much easier to arrange things sequentially or logically after the fact as I will at some point downstream.
WEDNESDAY, APRIL 26, 2023 (C DAY +86)
Tomorrow is treatment five (of six.) Then, after the last treatment a week from tomorrow, I have a month and a half break before getting scoped again. At that point, we’re back to zero because I’ll be “restaged” based on what my urologist/oncologist observes when she goes back in. It will be a new ballgame.
Not much to complain about. Sometimes my mind feels sluggish and I’ve had some fairly mild headaches behind my eyes. I know I haven’t been sleeping well on some nights. I’m trying to imagine what other cancer patients are dealing with when they are on radiation or IV chemotherapy. Thankfully, my imagination is stunted a bit as well at the moment.
Deena and I have casually discussed a trip Sloan Kettering or Massachusetts General for a second opinion, but we’d probably have to take a train to get to NYC and Boston is a good 3-4 hours drive. Would we go for just a records review? A full work-up (including cystoscope?) If I needed a cystectomy and it was performed at some distance from where we live, would we have to have follow-up care thereor could it be done locally?
THURSDAY, APRIL 27, 2023 (C DAY +87)
Doing okay today. Chemotherapy at 1:00 p.m. I’ve been thinking about how one thing can signal the end of something, but if you look beyond that “thing,” it can also signal a beginning of something else. Take the famous painting below:
This painting depicts the forces of British Major General Charles Cornwallis, 1st Marquess Cornwallis (1738–1805) (who was not himself present at the surrender), surrendering to French and American forces after the Siege of Yorktown (September 28 – October 19, 1781) during the American Revolutionary War. This battle is thoufght to represent the end of the American War of Independence. Public Domain. This work is in the public domain in the United States because it was published (or registered with the U.S. Copyright Office) before January 1, 1928.
To the British and loyalists in America, this event was a tragedy. It marked the end of British dominance in the colonies and the rnd of the American Revolution. But it also represented the beginning of something else: The birth of a nation. And this nation that was born came to the aid of England numerous times afterwards and today is a steadfast ally of Great Britain.
FRIDAY, APRIL 28, 2023 (C DAY +88)
Restless night after the fifth treatment, which could have gone better had the regular staff been present. Around 1:30 a.m. I woke up and was very tired, but felt too yucky to sleep. I’m not sure why or how, but with each treatment I feel a but more washed-out. Trying to recover today.
SUNDAY, APRIL 28, 2023 (C DAY +90)
Approximately three months since my first surgery. A quiet day today. With each treatment of chemotherapy it takes me half a day to get back to normal physically and in terms of my thought processes are concerned. One more treatment this coming Thursday, and then a six week period to let my bladder recover from the toxic meds (one of which–the Docetaxel–is highly combustible as a liquid and a gas.)
I sent out a post on the Nextdoor neighborhood app to see if there was anyone in the county (specifically men with cancer) who would like to meet for breakfast, lunch or brunch once a month. I should know in a few days if there is any interest. Even one or two others would be a start.
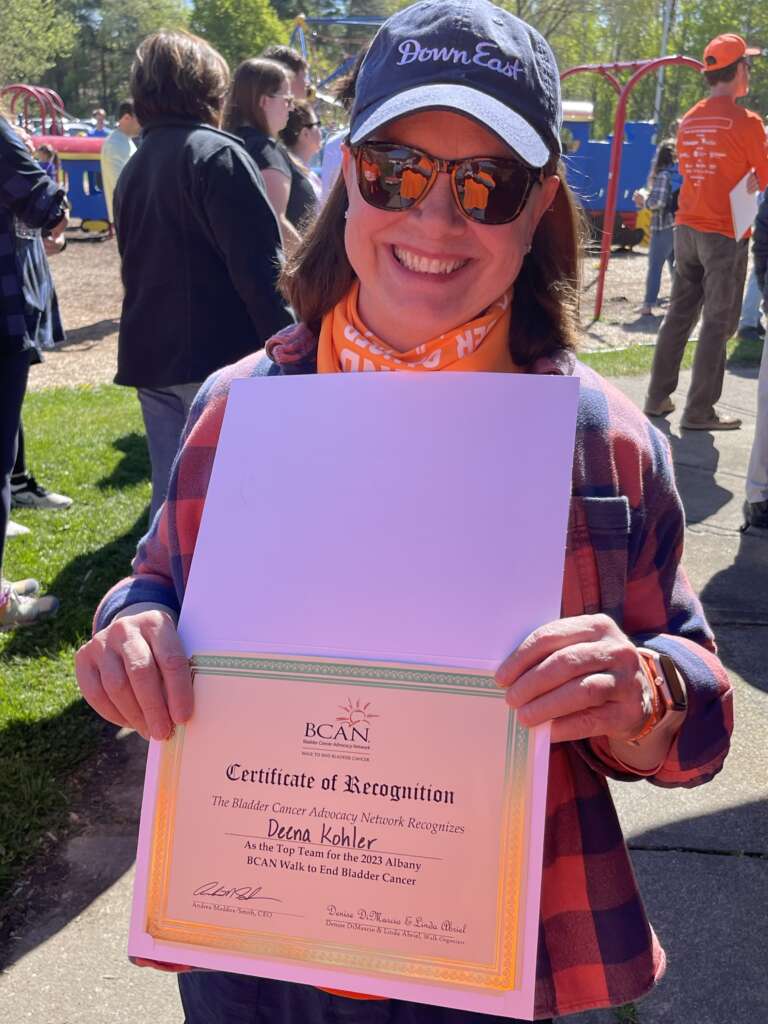
This Saturday is the Bladder Cancer Awareness Network (BCAN) walk which Deena and I will participate in. She has tirelessly involved herself and her many friends in contributing well over a thousand dollars in donations to the Bladder Cancer Awareness Network. Many of you have contributed as well, so “Thank you” fromthe bottom of my heart.
I’ll likely have little to post during the last three weeks in May, partly because we will be out of town for the last week. I’m hoping to start Part Five in June an improved format with new, fresh information.
THURSDAY, MAY 4, 2023 (C DAY +94)
Last day of chemo for a while. After my June visit with my oncologist/urologist for scoping and restaging, I will receive at least one more “maintenance” bout of chemotherapy with future scopes and bouts at three month intervals.
Board game courtesy of Printablee.
Last night I felt fairly stressed. Not about the future, but about today. I could see myself as one of the plastic, closed markers or figures in an old fashioned board game. Depending on the game, the players either spin a dial rapidly or roll dice to advance their markers. The number on the dial or the dice indicates how many spaces you advance. But while some spaces get you closer to finishing the game, other spaces on the board are marked “go back five spaces” or “miss a turn” or “start over.” There is little strategy in a game like this, just plain luck or fate which decides on what space your piece lands. So, on the eve of something worth celebrating (my last of six chemotherapy treatments), I instead felt powerless. So Deena–who barely slept herself last night–and I talked for a bit.
By the time Deena and I arrived at the clinic, I was in a cheerful state of mind, especially to see my usual practitioner in the room instead of a strange person. But I had to wait until someone was found who could or was willing to cath me. There was a nurse who processed me in when I arrived, but when he was asked in the hall to prep me for the treatment (including catherize me), he politely declined to do so, saying he never actually did it before and apparently wasn’t ready to attempt it today. With still “no joy” twenty minutes later, I questioned my nurse practitioner whether I should recruit someone willing to give it a try. A family member? A bored bartender? Maybe an Uber driver who watches Chicago Med on Wednesday nights and has secret dreams of going into medicine? But, they found some brave soul and with only a few painful protests from my prostate, this person managed to push, prod and poke the tip of the catheter into my bladder. I advanced five spaces.
I was told that the “dwell time” or time that the Gemcitabine (the first medicine) would be in my bladder was now only one hour, not two. That was fortuituous news for clinics like mine who had more patients than they could manage receiving chemo for bladder cancer. Nor did I protest. Now, the turnaround time was cut in half. While they say you shouldn’t–sometimes you should–look a gift horse in the mouth, and I plan to investigate this policy change shortly.
So, Deena and I rolled the dice again and the space we landed on said “Walk a marathon.” Or something like that. We’re headed to the Bladder Cancer Advocacy Network (BCAN) event this Saturday.
SATURDAY, MAY 6, 2023 (C DAY +96)
We attended the BCAN event with Deena’s sister Debbie and a mutual friend (Delores.) There were about 100 people at the event. I met two other vets with bladder cancer and there were doubtlessly many more people attending whom I did not know. Deena received an appreciation certificate for raising almost $1,500 for BCAN and BCAN’S outreach to bladder cancer patients. My doctor and nurse practitioner were there, and their presence was appreciated. We took a turn on the circuit before leaving for home.
This entry will conclude this Part 4 post. I am in the process of reformating and consolidating the information thus far into a more attractive and accessible format.
From left. Penny (my NP) on my right and Dr. Bernstein my urological oncologist on my left.
So, we will be off for a lovely drive to Vermont on Tuesday, our second trip in a week. Hopefully we can find another beloved covered bridge in the doing and make the most of this serendipitous trip. dsk
When I read about the hoops the VA has you jumping through, I am so angry. Veterans should be honored and given top of the line treatment, not relegated to 100 miles of travel. I know you and Deena have the knack of finding the rainbows but still..
I will follow your travels and cheer you on while the anger festers in my soul.
It does seem strange. When I was evaluated for another issue last month, I had someone in the local veterans medical center only ten minutes from home ask me twenty questions about my health. Tuesday, Deena and I had to drive almost five hours (200 plus miles round trip) for another person to ask only half as many questions (and at the personal cost of a hotel room.) Why not do it over the phone? Telemed? Ask the doctor to sign a sworn statement? But then, the VA is a huge bureaucracy with almost 800,000 open claims on any given day and more piling in each day (plus those in appeal.) Some claims are more serious or urgent than others. The pandemic slowed things down, too. I’m sure there may be more efficient ways to process claims, but that might take an act of Congress to reform the VA and Congress isn’t doing very much at the moment. So, we just wait until our number is called. Thank you for your support, Janice.
Thank you for sharing your journey and keeping us updated! This breaks it all down! Thank you both for always caring for our kiddos and their medical needs, even while you go through this journey with cancer. We love you.
You have a great outlook! Glad you are still doing ok after your sessions.
Maybe Lebanese woman are smoking as a form of resistance, or its second hand smoke. I only had to look up one word this time. ? That was an interesting video, but it felt like I missed the end. Does the scrapped/burned piece get sucked up whole? Does it get broken down then sucked up?
Thank you so much! Good point about second hand smoke. The tobacco in that part of the world is pretty strong.
So, the procedure to remove a bladder tumor actually involves a sophisticated instrument called a resectoscope, not a cystoscope per se. The resectoscope has different “channels” or lumens to the tubing to pump solutions into the bladder while at the same time draining other cellular debris (such as cancerous “scraps,” blood and so on) through an outflow lumen or passageway. The resectoscope can also maintain a certain pressure in the bladder during surgery (particularly low pressure which is necessary to reduce swelling.) The scope has a light and an electric or laser “loop” that slices the tumor into pieces that are then drained or suctioned through one of the outflow lumens in the resectoscope. Resectoscopes also have forceps to grasp tissue. Ta daa!
Just a suggestion, could you start a new link to part 5? This one is getting lengthy. Maybe with a hopeful picture of finishing round 6 ! I love your writing. You’re brilliant.
You are my hero. I’m a blessed woman to have you right beside me. Let’s try to enjoy every day off from this roller coaster ride. Hold my hand. I’ll be with you always!
Your girl



















Janice Hite
March 20, 2023Keep posting, Ron, you are teaching me so much about caring and love.
admin
March 20, 2023Thank you so much Janet. I’m just a novice when it comes to caring and loving.
Deena Suzan Kohler
March 23, 2023So, we will be off for a lovely drive to Vermont on Tuesday, our second trip in a week. Hopefully we can find another beloved covered bridge in the doing and make the most of this serendipitous trip. dsk
Janice Hite
March 30, 2023When I read about the hoops the VA has you jumping through, I am so angry. Veterans should be honored and given top of the line treatment, not relegated to 100 miles of travel. I know you and Deena have the knack of finding the rainbows but still..
I will follow your travels and cheer you on while the anger festers in my soul.
admin
March 30, 2023It does seem strange. When I was evaluated for another issue last month, I had someone in the local veterans medical center only ten minutes from home ask me twenty questions about my health. Tuesday, Deena and I had to drive almost five hours (200 plus miles round trip) for another person to ask only half as many questions (and at the personal cost of a hotel room.) Why not do it over the phone? Telemed? Ask the doctor to sign a sworn statement? But then, the VA is a huge bureaucracy with almost 800,000 open claims on any given day and more piling in each day (plus those in appeal.) Some claims are more serious or urgent than others. The pandemic slowed things down, too. I’m sure there may be more efficient ways to process claims, but that might take an act of Congress to reform the VA and Congress isn’t doing very much at the moment. So, we just wait until our number is called. Thank you for your support, Janice.
kelly
March 31, 2023Opa,
Thank you for sharing your journey and keeping us updated! This breaks it all down! Thank you both for always caring for our kiddos and their medical needs, even while you go through this journey with cancer. We love you.
Debbie C-M
April 25, 2023You have a great outlook! Glad you are still doing ok after your sessions.
Maybe Lebanese woman are smoking as a form of resistance, or its second hand smoke. I only had to look up one word this time. ? That was an interesting video, but it felt like I missed the end. Does the scrapped/burned piece get sucked up whole? Does it get broken down then sucked up?
admin
April 25, 2023Thank you so much! Good point about second hand smoke. The tobacco in that part of the world is pretty strong.
So, the procedure to remove a bladder tumor actually involves a sophisticated instrument called a resectoscope, not a cystoscope per se. The resectoscope has different “channels” or lumens to the tubing to pump solutions into the bladder while at the same time draining other cellular debris (such as cancerous “scraps,” blood and so on) through an outflow lumen or passageway. The resectoscope can also maintain a certain pressure in the bladder during surgery (particularly low pressure which is necessary to reduce swelling.) The scope has a light and an electric or laser “loop” that slices the tumor into pieces that are then drained or suctioned through one of the outflow lumens in the resectoscope. Resectoscopes also have forceps to grasp tissue. Ta daa!
Dee
April 28, 2023Just a suggestion, could you start a new link to part 5? This one is getting lengthy. Maybe with a hopeful picture of finishing round 6 ! I love your writing. You’re brilliant.
Dee
May 4, 2023You are my hero. I’m a blessed woman to have you right beside me. Let’s try to enjoy every day off from this roller coaster ride. Hold my hand. I’ll be with you always!
Your girl
Ron
May 4, 2023You are my angel and always at my side through thick and thin!