The very beginning of my cancer blog can be found here
JUNE 11, 2025 (WEDNESDAY)
Just received my first pathology report (on the two dimensional tumor scrapped from my bladder):
“Final Diagnosis:
A. Bladder, Posterior wall, Biopsy:
Benign urothelium with submucosal fibrosis, favor treatment effect.”
The word “benign” jumps out, of course. Submucosal fibrosis refers to scar-like tissue beneath the urothelial lining, usually caused by chronic inflamation, radiation or (in my case) prior surgery.
The phrase “favor treatment effect” on a pathology report means (per Pathway MD):
“the observed tissue changes are most consistent with the effects of prior therapy, such as chemotherapy, radiation, or surgery, rather than indicating active disease or recurrence.”
Technically, there is a second pathology report to be released on the muscle specimen taken to ensure there are no cancer cells hiding there. But my urologist is not concerned about that prospect. I see her next week. Will write again then.
JUNE 4, 2025 (WEDNESDAY)
Well, the bottom line is that I had a small (~ 1 cm) tumor, likely to be cancerous removed from my bladder yesterday.
And actually, except for waiting a number of hours to get inside the main OR, everything went well. Because of my difficult airway anatomy which has been morphed by COPD or some other thing (including old age), the anesthesiology department recommended a spinal which I accepted (in my experience and opinion, it is generally foolish to not go along with professional advice concerning surgery.) However, once we got into the theater and I kept yaking away and offering my favorite life hacks to no one of the six people working on me in particular, they gave me an IV cocktail of Midazolam, Propofol and Fentanyl to put me to sleep anyway.
They did not do the blue light for some reason, chosing to just resection anything that looked remotely suspicious. The tumor they found was described as a one centimeter (four tenths of an inch) sessile tumor. According to Parthway MD, this is a “flat, broad-based lesion attached directly to the bladder wall. It is basically only two dimensional (length and width) like an oil stain on the garage floor which is why the CT n April idid not notice it. Furthermore, it was classified as cT1 stage, which means “that the cancer has invaded the connective tissue beneath the bladder lining (lamina propria) but has not yet reached the muscle layer of the bladder wall. It is a non-muscle-invasive stage that hasn’t spread into the deeper tissues of the bladder.”
So, the tumor was biopsied and removed and the muscle tissue was also biopsied to be sure there are no cancer cells in the muscle. If there are, they will advise me to have my bladder removed. The good news is that they found a way to anesthesize me for future surgeries and that the procedure went well. And, though is seems like the cancer returned, it also seems like it was caught just in time, though we won’t know for sure until the pathology report confirms that the muscle tissue is clear from cancer.
So right now, I have a urine collection bag attached to a catheter. Thank God I have no pain. I know many people do hurt and if I hurt inside, it is for the 43 y.o. men and the the 32 y.o. single mom’s with small children who are in my shows.
Catheter comes our tomorrow. More to follow~
TO MY MANY FRIENDS, SUBSCRIBERS AND FELLOW PATIENTS
I have many people each week from many different countries who read my cancer blog. My focus is usually on the physical challenges of the disease. But there are other dimensions as well, such as the psycho-social, the spiritual and even the financial (costs of cancer.) As someone who is your everyday, garden-variety Christian, I do want to leave you with a brief message and hopefully you will not feel pressured one-way or another.
The invisable hand. Credit: Shutterstock.
I have a peace with where I am. Of course, I have the luxury of being just a few years from turning 80. My children are grown and I enjoy time with my grandkids when I see them because some of them live in different states. I lost a wife who I loved and remarried another woman whom I love. I do believe that God is taking this cancer journey with me. I also know that even if I had perfect health, at my age, I would probably leave this life before you do. I might not have this peace if I had unfinished business or things that I still need to accomplish. As the poet Robery Frost once wrote:
“But I have promises to keep,
And miles to go before I sleep.”
I believe that God has helped me in this battle, but I see loving, heroic people around me who have fallen. Why were they not given more time? The truth is I don’t know. But if my oncologist told me that I only had a few weeks left to live and would likely face a painful death, I would not regret the choice I made years ago to embrace my Creator.
God bless you all!
JUNE 3, 2025 (TUESDAY)
Today, I have a second attempt at my third TURBT. It’s been two weeks since the failed attempt described immediately below. Today, it will be in the Main OR on the university medical campus. I have to report at 11:00 a.m., so I will probably be sent to OR around 1:00 p.m. since I have to have the Cysview contrast in me for one hour before the procedure, and then there is also the time needed to check me in, sign consents start an IV, etc.
I only got perhaps three hours of sleep last night. I was wondering what I’d be like tonight. I rather expect to have a catheter when I come home given my blood clot problem during my second TURBT when I could not urinate. I did have a catheter for my first TURBT following discharge. I also wonder whether there will be much pain afterwards. So far since I was diagnosed, it has been very tolerable, but I know some bladder cancer patients report significant pain. Today will be the fourth time in a year I’ll be put to sleep. THe last few times I’ve had a moderate amount of pain in my next and jaw from the endotrach inturbation. When I was much younger, this was not as much of a problem. Perhaps when you are in your seventies your nasopharyngeal anatomy is not as pliable. It might be nice to spend the night in the hospital just be sure everything is okay before discharge, but that likely will not happen unless my urological surgeon deems it necessay after she goes in. So, Deena and I prayed about it. God’s will be done. More to follow.
MAY 20, 2025 (TUESDAY)
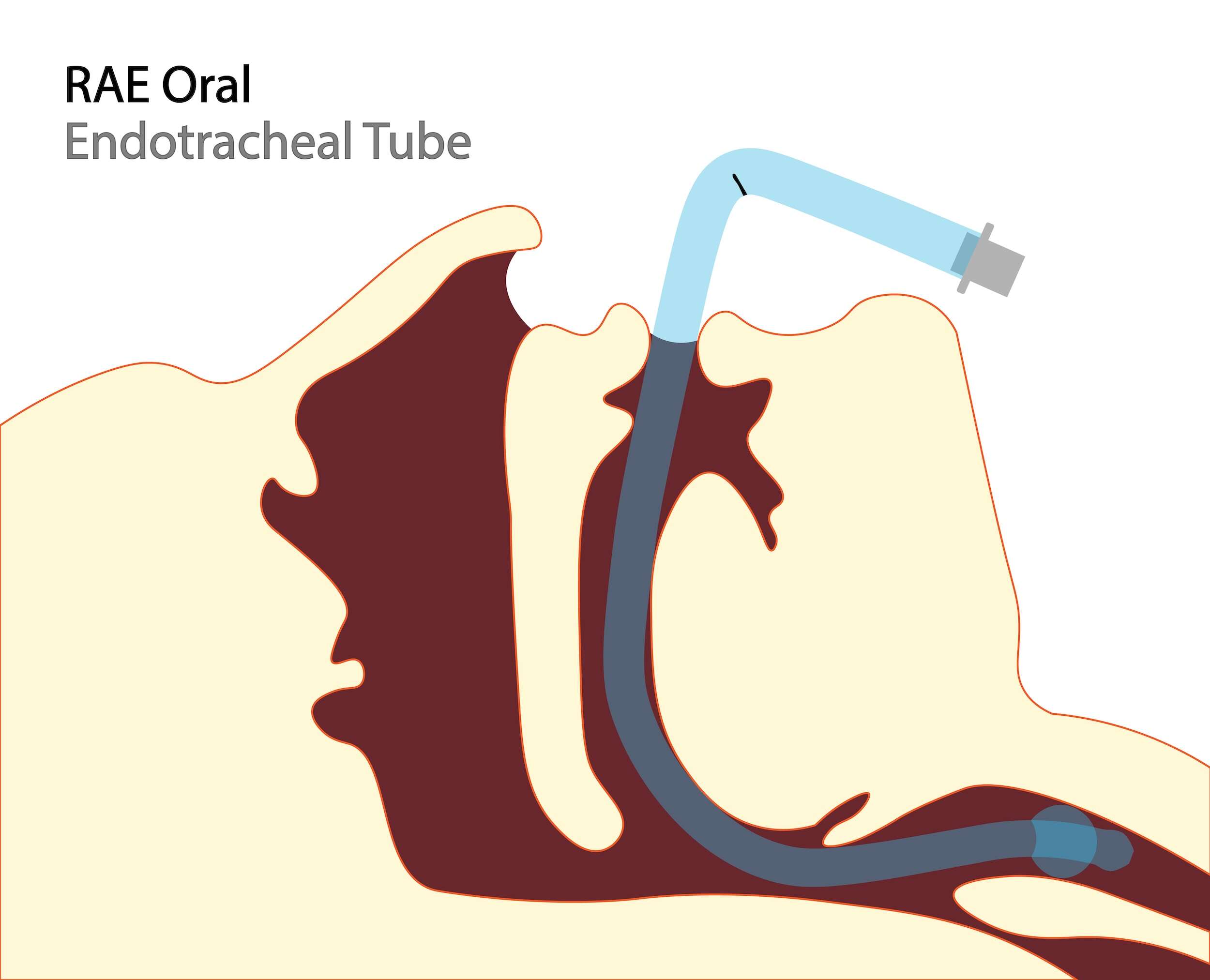
Oral endotracheal tube. Credit: Jennifer Fontan (iStock.)
My post from yesterday (immediately below) revealed that my surgery was postponed after I was under at least some sedation (at least enough so I wasn’t aware of, or able to gag from, tubes being slid down my throat.) The reason the surgery was scrubbed was that there was either swelling or extra tissue buildup or some sort of injury that narrowed the passageway to my lungs since my last surgery nine months ago. My surgeon believes that a second attempt at the main hospital OR will succeed for several reasons including a wider selection of instruments, so I’m in favor of that. Another option for a TURBT would be a spinal and then there are yet more tricks possible without an epidural or the like. But I’d like to get it resolved because next month I have a colonoscopy and will have to go through this all over again. And who wants to prep twice for a colonoscopy?
Some of the causes of airway obstruction include COPD (particularly asthma), obstructive sleep apnea, tumors, changes in the muscle mass and changes in body weight. The use of ultulrasound and certain video probes can be used to surveil a way to the proper positioning the endotracheal tube, and these may be some of the compliments that only larger facilities have (hence the reason why I’ll have it done there.)
MAY 19, 2025 (MONDAY)
We went in this morning for my first blue light cystoscopy. I went through the typical check-in procedures, consents signed, vital signs taken etc. They did check my fasting blood glucose level and it was 105. That’s the highest I’ve seen it in several years, though I don’t check it more than a dozen of times a year and then often when I’m hypoglycemic with low blood sugar, which is an emergency. With a 5.7 A1C because of Ozempic, I trust (and perhaps misplace my trust) in the work of the GLP-1 receptor agonist in the medication to keep my daily fasting blood levels down and my A1C will bear out whether this is so or not.
They started an IV and straight-cathed me to add the Cysview® contrast, then removed the catheter. Ninety minutes later the OR nurse, the anesthesiologist and my doctor stopped by. After that, I was transported to surgery. While my personal experience in the area where I live is that doctors and surgeons have practiced hands and excellent bedside manners, anesthesiologists can be a tad more forceful than need be as they practice their skills. Perhaps they need to be, but it seems it is comparable to having an IV inserted. Some nurses can slip one in and have it secured before you can say “Ow!” Other nurses take five tries, each more painful than the one before it.
So, the anesthesia team put a very rigid mask over my nose and mouth. This was not the soft, mint green plastic mask patients on the units know, but a mask with a hard border. It was particularly painful across the bridge of my nose and I wound up with a bruised lower lip. Eventually I fell asleep and woke in recovery. When I asked how things went, I was told “not well.” The procedure was called off because the anesthesiologist could not inturbate me (i.e., insert an endotracheal tube patently.) Their report said that my internal anatomy had “changed” in the last year since I was inturbated and these changes made it impossible to inturbate me safely. As I pondered this, I was passing blood clots whenever I blew my nose and spitting up dark blood by mouth. The clinic is to reschedule my blue light cystoscopy/TURBT at the main campus OR at some future date (preferably soon.)
More to follow on this and other options tomorrow.
MAY 18, 2025 (SUNDAY)
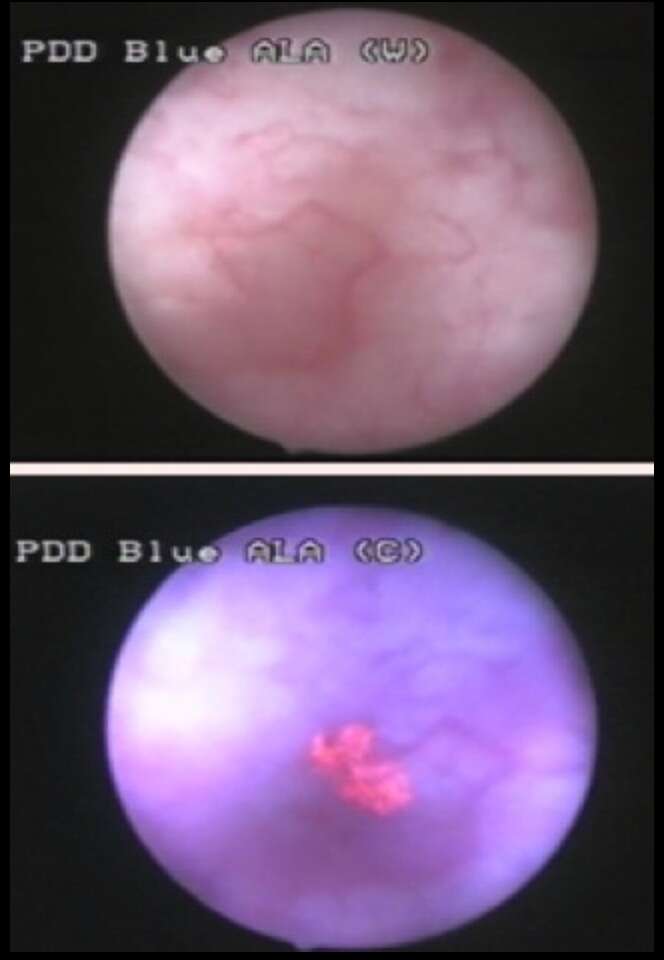
Pink area in the lower photo reveals cancer under bluelight. Credit: CC.
Tommorow morning, I have my third TURBT in twenty-eight months. Maybe. Officially it is a blue light cystoscopy, but I will be asleep for the procedure. However, my urologist seems concerned enough to go in and scope my bladder only three weeks after the last cystoscopy, so I expect the consent I sign tomorrow will include a TURBT if indicated. I’ve asked probably a hundred or more patients in the past to sign surgical consents myself when I worked med/surg. The toughest ones were for women who had a breast lump. They consent for the lump to be removed, and if needed, the entire breast, or both breasts maybe. So you are giving your doctor the freedom to act on his or her discretion. Like a blank check, which underscores the need for trust between patient and physician. I trust my doctor completely. The alternative would be for my doctor to wake me tomorrow after the cysto to tell me they need to do a TURBT–is that okay–and then to put me under anesthesia again? No way.
The “blue light” cystoscopy uses a special contrast, termed Cysview® (hexaminolevulinate HCl.) The solution is introduced into the bladder via catheter an hour before the procedure begins. It allows the doctor to visualize urothelial tissue that might otherwise appear normal or unremarkable. After the procedure, the contrast is remove through normal voiding.
I’ll report back as soon as I can after tomorrow’s procedure.
MAY 12, 2025 (MONDAY)
Getting a urine culture and sensitivity today as part of my pre-op clearance. Tomorrow I see my cardiology clinic for an EKG and quick exam and chart review. A week from today I have my procedure.
My bladder wash report came back today:
Bladder, washing:
Indeterminate
Atypical but degenerated urothelial cells.
“Atypical but degenerated urothelial cells indicate abnormal changes in the cells lining the urinary tract, which may suggest a precancerous or cancerous process.” Degeneration refers to “changes in the cells that could be due to various factors, including inflammation or injury” according to Pathway MD. So, the cytology (examination of individual cells floating free in the bladder during my last cystoscopy) was not conclusive any more than the biopsy, and a TURBT is definitely indicated.
My TURBT will be under Level II or Level IV general anesthesia (most likely IV because of past issues where I have tried to move about while asleep.) That will mean I will probably be intubated with an endotracheal tube because of my obstructive sleep apnea.
MAY 5, 2025 (MONDAY)
Got a cal from my urologist;ogist this afternoon. She plans a blue-light cystoscopy/TURBT under sedation on the 19th of this month to positively rule out/rule in urothelial cancer. This will be my third in two twenty-six months. It’s the cost of two year sof quality living, and I’d gladly suffer it. You are put to sleep, wake up, catheter out and if you can void (urinate), they cut you loose. This time, however, we plan to hang around the hospital for a few hous because the last time, I had to be transported to the ER via ambulance less than two hours after catheter reemoved because of a blood clot occluding the uretha.
MAY 3, 2025 (SATURDAY)
My pathology report went up overnight. Here is what it noted:
Final Diagnosis:
A. Bladder, posterior wall, Biopsy.
Scant fragment of urothelial mucosa with focal atypia, cannot entirely exclude urothelial carcinoma in situ. See comment.
Comment:
Scant nature of the specimen hinders further evaluation.
Gross Description:
The specimen is labeled “bladder biopsy”: Received in formalin is an irregular, soft, tan tissue measuring 0.1 x 0.1 x 0.1 cm which is entirely submitted in a single cassette labeled A1.
Focal atypia, in the context of pathology, refers to “localized or limited instances of atypical (nontypical) cells or tissues within a large tissue sample. It’s a qualitative descriptor indicating that while abnormal changes are present, they are not widespread or affecting the entire tissue” (Apple AI.) Urothelial carcinoma in situ is a “high-grade, non-invasive cancer with a potential for aggression and recurrence. It requires careful diagnosis and management, with intravesical therapy being the preferred treatment option” (Pathway MD.) My wife and I understood this to mean that the specimen size was not adequate to ensure that enough cells were available to determine the presence (or absence) of cancer. We are thinking that we’ll be contacted after the bladder washing cytology is completed about some sort of follow-up procedure, possibly a TURBT, but we have no way of knowing what course our urologist might choose.
MAY 2, 2025 (FRIDAY)
I had a scheduled cystoscopy on Wednesday. I was able to observe the screen as she proceeded. My urologist, whom I have complete confidence in revisited one of several inflamed areas of bladder. She appeared troubled or mildly concerned. She asked me if I consented to a biopsy and I said “Certainly.” She did a biopsy six months ago which came back negative. She had her assistant inflate my bladder with what I suppose was sterile saline. This causes the bladder to distend or stretch, which makes any lesions (abnormalities) more visible as well as allowing making the scope even more wieldy, which is probably not the best word choice here. I watched her excise two specimens of tissue, and it left three or four areas in the bladder wall that bled minimally. It appeared to me like I was in a plane flying over several small volcanos that were smoking (the smoking appearance caused by the release of blood in the solution.) She then zapped each spot with electrocautery or a laser. There were several orange-colored flashes from the end of the scope visible on the screen as she concentrated at the point each “smoke-like” trail of blood emerged from the bladder wall as she “zapped” each spot. As she withdrew the scope, she mentioned that I might have a tiny bit of bleeding in my urine which I did not. I asked her if her biopsy was out of an abundance of caution. I wondered whether that was a fair question to ask. On the one hand, my wife and I have come to trust her completely so there was a reason she had to decide to perform a biopsy. On the other hand, without a pathology report, no one can know for certain which is going on. She did schedule my next biopsy for October, but said that she might have to move that up, and she hinted (or I understood that she hinted) I might need a another TURBT this summer. She mentioned she noted a small change in one of the areas she biopsied compared to what she noted earlier this year. One the other hand, it has not “blossomed” as she described it.
Of course, my wife and I are fairly anxious about what the pathology on the specimens and the cytology on the bladder wash might show. We had some trips planned this summer with the family and disrupting those activities was a concern. The CT from two weeks ago did not notice anything alarming when compared to earlier scans, but then while a CT is necessary, it is not always sufficient (hence the cystoscopy.) My wife Deena pointed out that my last chemotherapy treatment was only six weeks ago, so if there is a return of my cancer, it likely began earlier this year while I was still receiving Gemdoce. I know from my biopsy last fall that the report may come back normal, but I also know that I have high grade urothelial cancer so I should not be surprised if and when it does return. I have read accounts from other patients with my type of NMIBC that have gone through this cycle for ten years or more; getting a pathology report that reveals cancer and then a TURBT every few years and going on and off some sort of other treatment available (and there have been some new ones developed during the last few years.) But they still have their bladders. At the age 76, I’d be happy to have another decade, though something else might shorten my life expectancy before I reach the downside of 90 other than bladder cancer.
Tomorrow is the annual BCAN fundraising walk. If you are unfamiliar with this organization, it is a valuable, easy to understand website with tons of videos explaining procedures, interviewing surgeons and urologists on bladder cancer and so on. I strongly encourage you to visit that site if you are unfamiliar with bladder cancer.
“CYSTOSCOPY with biopsy/fulguration Preoperative Diagnosis: Bladder Cancer FINDINGS: The anterior urethra appeared: Normal. The prostatic urethra appeared: Normal . The median lobe was Present. Small
The ureteral orifices were Normal. Bladder neck was Normal. The bladder appeared Abnormal There were areas of erythema noted at the posterior bladder and right lateral wall. Area of erythema at posterior bladder was biopsied.
Trabeculations noted: Yes
Diverticuli noted: Yes. Small. Noted near dome, explored with normal appearing mucosa. There were no foreign bodies. Cytology sent: Yes Biopsy performed: Yes Urine culture: No
ASSESSMENT:
High risk non-muscle invasive bladder cancer (Hg Ta>3cm)
– Participating in clinical trial randomized to gem/doce
Completed gem/doce induction and maintenance
–Per research protocol, No further maintenance Gemzar/docetaxel needed.
– Next surveillance cystoscopy y 6 months thereafter per research protocol.”
APRIL 15, 2025 (TUESDAY)
A month now since chemotherapy was stopped. I had a CT-can yesterday which noted once again “bladder wall thickening.” Thickening of the bladder wall can be caused by infection (e.g., cystitis); infections such as TB; obstructions; bladder stones and cancer. Thickening of the blader wall can make it difficult for the partient to completely empty their bladder. In the case of bladder cancer, the cancerous tumor “pads” the bladder wall either along the inner lining of the bladder, or as it spreads inward to the other layers in the same area. But in the ten months since my last CT-Scan, all the radiologist could remark was”No significant interval change.” That tells me there is nothing going on and it is akin to scar tissue, though that analogy is incorrect.
At the end of the report the radiologist thconcluded with words: “No evidense of metastatic disease in the abdomen and pelvis.” I’ll take it.
MARCH 16, 2025 (SU)
I showed up for my monthly chemotherapy on Friday and my Nurse Practitioner came out to the waiting room to greet me with a card and a balloon. She knew it was my birthday. She was particularly anxious for me to open the card and when I did, there was a certificate saying that this would be my last round of chemotherapy (I was getting Gemcitabine and Docetaxel for the last two years. I understood that my last monthly treatment would be this June, but apparently, I meet the criteria of the American Urological Association which provides treatment recommendations for bladder cancer to clinics and hospitals across the U.S.) I was shocked, to say the least. In fact, it took me a day and a half to get used to the idea. Ordinarily, a celebration might be in order, but after two years, the chemotherapy had become something of a life preserver for me as I was tossed about in choppy waters over a deep, unfathomable abyss from which few return. Now all of a sudden it was like I had to stay afloat without any assistance.
I want to repeat my initial staging and some other pertinent information to summarize. Obviously, in some practical sense the staging is not relevant any longer (i.e., I no longer have a tumor larger than 3 cm), but in another sense, it is still important because the pathology identified high grade cancer following my TURBT which suggests that the cancer may reappear in the future.
So, I have (had) Hg Ta>3cm. This is urothelial cancer [which] “refers to a non-invasive but aggressive form of bladder cancer that involves the urothelium without invading the muscle layer.” A second pathology performed in February 2023 on tissue from a different part of my bladder following a second TURBT revealed “pT1 high-grade papillary urothelial carcinoma” and “LG Ta MP present w/o cancer.” The term:
“pT1 high-grade papillary urothelial carcinoma” is a type of bladder cancer characterized by tumors that invade the lamina propria (pT1) and exhibit high-grade histological features, indicating a more aggressive behavior and higher risk of progression. The lamina propria is a layer of connective tissue located beneath the epithelium of mucous membranes, playing a crucial role in supporting the epithelium and housing blood vessels, nerves, and immune cells Pathway. High-grade tumors are more likely to progress to muscle-invasive disease and metastasize. There is a significant risk of recurrence, requiring close surveillance and management.[1]”
In these cases, Bacillus Calmette-Guérin (BCG) is the gold standard, but there is not enough BCG to go around up in the Northeastern region of the U.S.. I was given an outside chance to get BCG by participating in a clinical trial, so I signed up for it. However, I was not selected to receive BCG but Gemcitabine and Docetaxel (Gem Doce) instead. As it turns out, Gemcitabine and Docetaxel provides almost identical effectiveness as BCG but without the side effects of BCG as BCG provokes an immune response in the person receiving it.
Low-grade Ta multifocal papillary (LG Ta MP) bladder cancer is a “non-muscle-invasive bladder cancer characterized by multiple low-grade papillary tumors confined to the urothelium without invasion into the bladder wall.”
From here on out. I expect to receive two cystoscopies a year and one or two CT-scans. This will be the only surveillance performed. However, I plan to check my urine for blood regularly since that is often the first sign of a recurrance of bladder cancer. Am? I cured. My urologist might be had to pin down on that question. In one sense,a patient is considered “cured” if the can go for five years without another episode of cancer. Some ocologists would say that a cancer patient is potentially never cured, if only because their DNA has been corrupted.
So, how am I physically? Physically, I’m doing ok for someone 76 years old with other co-mobidities, such as early Parkinsons Disease. I have my PSA checked each year for signs of prostate cancer but so far, so good. I can go all day without an “accident,” but out in public, I rarely use urinals anymore. This is because when I urinate and reach the point where I lose the sensation to urinate and I feel like my bladder is empty, it is actually only half so. It takes several more tries of contracting my pelvic muscles to empty it completely, and that is where an accident is most likely to occur. On road trips, I usually wear or bring along some incontinent product like Depends. At night, I some time have a few drops of urine on my night clothes, so at least once a week in the middle of the night I’ll change.
I’ve only had one urinary tract infection over the past twenty-four months. Given the fact that probably seven or eight different nurses and/or techs catherized me over the past two years, not counting the six or seven cystoscopies that I had speaks pretty highly of the outpatient clinic where I get my treatments. Nor can I be certain where the UTI occurred. I felt pretty ill during that time at home and I was on two different antibiotics. But I may have been battling a touch of the flu as well, I don’t recall.
Compared to people with other types of cancer and going through other treatment modalities or circumstances (e.g., radiation for advanced breast cancer, people with metastisis to their liver or lungs, and bladder cancer patients who have lost their bladders, I feel very fortunate, humble, and I understand that someday I may be joining their ranks.
I cannot overstate the role of faith and prayer in my experience over the past twenty-six months. We have all likely known someone struggling with cancer or some other life threatening ordeal. Possibly, we prayed for them as they did for themselves and quite possibly or even more than likely, they succumbed to their illness in spite of this. Nor can we test the usefulness of faith and prayer in a clinical trial or setting like we can with a drug or a procedure. But a person’s state of mind, the presence (or absence) of support systems, the patient’s general health, etc. no doubt all factor into the equation. So, while I cannot quantify the usefullness of faith and prayer and while I cannot offer any guarantee in your struggle, I firmly believe that it was to my benefit to rely on it in mine. Elsewhere on my blog you can find useful information about faith and prayer and if you contact me, I will be glad to share my personal experience.
I plan to launch a new cancer thread in the next week or so with more information on bladder cancer. I’ll link it up from here for your convenience. Please stand by.
Today, I received the bladder washing report from my cystoscopy of January 29th (discussed below.) A bladder washing is the last thing the urologist does before she removes the cystoscope. It involves injecting a sterile solution into the bladder and then suctioning it out via the cystoscope and draining it into a speciment container. The objective is to collect whatever stray cells may be floating around in the bladder and provide a sample for the cytologist to examine. My report came back:
Bladder, washing:
Benign
Reactive urothelial cells
So, the good news is the word “benign.” All the cells examined were noncancerous. But what are reactive cells? According to Pathway AI, a popular decisionmaking app among residents:
“Reactive urothelial cells are a type of epithelial cells from the urinary tract that have undergone changes in response to inflammation, irritation of injury. These changes can include alterations in cell size, shape or nuclear features. Injury, infection, kidney stones, catherization itself, chemotherapy or radiation can all produce reactive cells.”
But, so can cancer. When my urologist received this report, she likely noted the word “benign,” but then saw “reactive urothelial cells.” At this point, I imagine she reviewed her notes and any photos she took from my cystoscopy last week to see if there was any sign of cancer. If not, then the most likely explanation is that these reactive cells correlate with her finding of erythema (inflammation), and in the absence of pain or blood in my urine, she concluded that I am doing well and appear to be cancer free for the moment. Tomorrow I have my nineteenth chemotherapy treatment.
JANUARY 29, 2025 (W)
Two years ago tomorrow, I had my first TURBP for high risk, non-muscle invasive bladder cancer (Hg Ta>3cm.). Today, I had my eighth cystoscopy and, thanks be to God, there was no sign that the urothelial cancer had returned. Specifically, the report reads:
FINDINGS:
“The anterior urethra appeared normal; The prostatic urethra appeared moderate; The ureteral orifices were normal; The median lobe was not prominent; Bladder neck was normal; The bladder appeared normal with posterior erythema; There were no mucosal lesions suspicious for neoplasm; There were Grade 1 trabeculations; Bladder diverticuli were not noted; There were no foreign bodies;; Cytology: Yes Biopsy: No; Location: not applicable; Culture: No.
Cystoscope was removed and patient tolerated procedure well.”
The comment on the prostatic uropathy could refer to the size, shape, or degree of obstruction in the prostatic urethra. There may have been an issue common to 75 y.o. men like myself called benign prostatic hypertropy (BPH) which means that the chestnut-sized prostate gland has enlarged and thickened somewhat, therefore squeezing the urethra which it surrounds. Or, it can refer to urethral strictures. Strictures can be caused by repeated cauterization of the bladder, of which I’ve had twenty-four or so catherizations. This can lead to scar tissue blocking the urethra which conveys urine from the bladder to the outside of the body. But at the moment it does not seem to be worrying. The “erythema” noted is most likely due to inflammation. My urologist thought about it for a moment and decided to just watch for it three months from now since (a) there was nothing really to biopsy and (b) shes has seen my bladder in worse shape. She did tell me she was very pleased about the way I’ve responded to the continuing Gemdoce (chemotherapy.)
This remark led my wife Deena to ask her why, in that case, will the chemotherapy stop this July after twenty-eight months. There were several reasons. First of all, over time, urothelial cancer develops a resistance to gemcitabine and docetaxel, and it can be plotted as a certain percentage a month. Also, new generations of cancer cells may have this same resistance. Another reason to stop chemotherapy is cost.
If and when Gemdoce is no longer effective, there are second line drugs to try. Overall, my urologist says she was very pleased that my cancer has responded as well as it has. For this, I give thanks to God, for making this treatment available to me when so many other people around the world cannot access the drug and for the success my body has enjoyed in resisting the cancer, something that not every body has.
She also sent a specimen of the bladder washing solurion to cytology.
JANUARY 17, 2025 (F)
Clinical Scoring
Just over two years ago I was scheduled to have an abdominal hernia repaired. When I was in my twenties and before laparoscopic surgery was as common as it is today, I needed abdominal surgery. The surgeon cut a twelve-inch incision from the tip of my sternum (breastbone) to my navel. Over the decades, the incision started to herniate, creating a slight bulge near the bottom of the scar. A surgeon I saw in 2022 recommended repairing it, which meant another surgical procedure. I had to see a doctor for “pre-clearance” first, however. This was something new to me. I don’t know if it was because I was over seventy, or if it was something that the insurance companies now required of people of any age. Perhaps it was the medical canons and some new standard of care? So, I was ordered to make a surgical pre-clearance appointment, where for the better part of an hour, a physician asked me dozens of questions, entering my answers in his laptop as quickly as I responded. Suddenly, it was clear to me what he was doing. I asked him “Are you running an algorithm on me?” He responded sheepishly that he was. At the end of the interview and a subsequent cursory exam (which included an EKG and bloodwork accomplished in advance of the appointment), he came up with a numerical score and said I was a good, though not a perfect candidate (risk) for the surgery. The score was based on my medical history, my answers to his questions and my lab values as well (cholesterol, A1C, creatinine and kidney function, weight and height, etc.) Left unsaid was what would have happened if I was not a good candidate for surgery?
Cancer patients are no strangers to surgery or other expensive or painful procedures. Bladder cancer is the most expensive cancer to treat in America for reasons I mention elsewhere in my blog. No two patients are identical. Urologists and oncologists must decide whether to recommend one treatment or another. Should an eighty-nine year old man receive radiation on his prostate? Should a thirty-two year old woman with two young children have her bladder removed? What if she’s pregnant in her first trimester? What about a thirty-two year old woman without children but with a history of substance abuse? What about a homeless person? Probably, because healthcare is so expensive, insurance companies want to minimize costs and because surgeons are so stretched timewise, there needs to be some prioritization or ranking in their decision-making. So, I want to discuss three common tests today that you may or may not encounter. And even if you are not quizzed as extensively as I was, they may still be applied to you. Or not. Each in its own way is a screening exam. Keep in mind that these are only several tools among many that doctors may refer to. Nor are the tests likely to be the final word in any given case. They are often based on artificial intelligence, which still requires a human to weigh in on any recommendations.
The tests I want to mention here are the Clinical Frailty Scale, the Karnofsky Performance Status (KPS) and the American Society of Anesthesiologists (ASA) Physical Status Classification. These tests either assess your current health or assist your doctor in predicting likely outcomes. Heart patients may be familiar with the American College of Cardiology (ACC) Cardiovascular Risk Score. I have the app on my phone. There are additional rubrics as well, some more accurate than others, some built into the software that a hospital network uses. In many cases, a doctor or medical practice may not use a formal scoring system, but I personally think that from a risk management perspective, a scoring system might be a good thing.
Postscript: There are also grading systems whereby patients may grade their hospital in terms of services, safety and outcomes. The most common is a metric called Leapfrog, but Medicare also provides useful data to consumers.
Clinical Frailty Scale
As the name of the assessment suggests, this is an evaluation used for seniors; those with debilitating diseases, living in assisted living facilities or nursing homes, patients with various states of mind and so on. Patients are sorted into one of the following categories:
Clinical Frailty Scale Components (CFS):
Very Fit: People who are robust, active, energetic, and motivated. These people commonly exercise regularly. They are among the fittest for their age.
Well: People who have no severe disease symptoms but are less fit than category 1. They exercise or are very active occasionally, e.g., seasonally.
Managing Well: People whose medical problems are well-controlled but are not regularly active beyond routine walking.
Living With Very Mild Frailty: Previously named “Vulnerable,” While not dependent on others for daily help, symptoms often limit activities. A common complaint is being “slowed-up” and being tired during the day.
Living with Mild Frailty: These people usually have more evident slowing and need help in higher-order instrumental activities of daily living (IADLs) such as finance, transportation, heavy housework, and medication management. Typically, mild frailty progressively impairs shopping and walking outside alone, meal preparation, and housekeeping.
Living With Moderate Frailty: People need help with all outside activities and housekeeping. Inside often have problems with stairs, need help with bathing, and may need minimal assistance with dressing.
Living With Severe Frailty: Completely dependent for cognitive and physical personal care. However, they seem stable and not at high risk of dying (within six months).
Living with Very Severe Frailty: Completely dependent for personal care and approaching end of life. Typically, they could not recover even from minor illnesses.
Terminally Ill: Approaching the end of life. This category applies to people with a life expectancy of under six months who are not otherwise living with severe frailty. (Many terminally ill people can still exercise until very close to death.)”
Surgery always carries risks. I’ve cared for otherwise healthy patients who died unexpectedly during surgery. The cardinal rule in medicine is first do no harm. The CFS measures the potential for harm to a patient if surgery is attempted.
Karnofsky Performance Status (KPS)
The KPS evaluates a person’s health and provides a score from 0-100. If you rate 100, you are in perfect health. If you wind up with a zero, then you are declared dead. The KPS focuses on how well the patient can perform activities of daily living (ADL), such as caring for themselves, bathing, toilet needs, moving about their home and so on. A KPS score of less than 40 may predict a limited life expectancy. The KPS is similar in many cases to another evaluation called the ECOG Performance Status Scale (ECOG referring to the Eastern Cooperative Oncology Group.) KPS is used to evaluate patients for certain types of organ transplants, and along with the ECOG, are used by groups working with palliative care and hospice. This population includes patients with advanced-stage cancers as well. I’ll have a discussion on palliative care in the future. Note that in some of these rubrics, the data input is very objective, such as blood values, body mass index (BMI), age, blood pressure and so on. The data involves measurements that different people can agree on. And it can be repeated. Other tests rely on subjective data, meaning there is a certain amount of interpretation or filtering involved. Reasonable people in every case may not agree. For example, I may consider someone with an appearance of being intoxicated to be inebriated. You may not, however. A blood alcohol level test might indicate one of us to be correct and the other mistaken. And, in fact, if there is an appearance of alcohol intoxication, it might not be from alcohol at all!
An example of a test with numerous subjective components would be the American Society of Anesthesiologists (ASA) Physical Status Classification
This measurement instrument mentions, for example “Substantive functional limitations; One or more moderate to severe disease…”. Questions immediately come to mind, such as “What is a substantial limitation?” “What is a severe disease?” Also, “What constitutes a disease?” Certainly lupus (SLE) or T1DM (type one diabetes) would be a disease. But what about seborrhea or alopecia (baldness?). Would advanced alopecia be a reason to cancel surgery? Likely not. But, I may be wrong.
In my experience, an anesthesiologist has a tremendous amount of discretion when it comes to whether surgery is an option or not. They may even scrub a surgery after you’ve been admitted to surgical services.
So, these are just some of the more common tests. The usual caveats apply. The material I post on my blog is for general information only. Because I am not a physician, I cannot offer medical advice. Nor can I even guarantee that every single point I make is an accurate or a valid one. Whenever you have doubt, always consult your physician.
JANUARY 15, 2025 (W)
I have another week to go before my next cystoscopy, but I wanted to include some more information on bladder cancer. I thought today that I’d go into the very beginning of when bladder diagnosis was first diagnosed and I also want to share a bit about the urothelium of the bladder and urothelial cancer.
BLADDER CANCER APPEARS IN THE HISTORICAL RECORD
Credit: Natalia Babok
Bladder cancer likely existed long before recorded medical history. So, when was the first recorded case of bladder cancer? It is tricky nailing the answer to this question down. Some authorities cite Hippocrates (460 BC-377 BC), and while he was something of an authority on cancer (specifically breast and stomach cancer), and while he did talk about the importance of urinalysis to a medical diagnosis, he never specifically mentioned bladder cancer. Other sources credit Andreas Vesalius (1514-1564.) However, like Hippocrates, Vesalius did not specifically mention bladder cancer, either.
It is possible that a physician or anatomist in the sixteenth century “discovered” bladder cancer, but if so, that information is lost. Yet, people developed signs and symptoms consistent with bladder cancer, so doctors and surgeons knew that something was amiss. Sixteenth century medical treatment for cancer (at least as far as bladder cancer was concerned) called for compression. It involved applying continuous, physical pressure on a tumor with the hope or expectation that the pressure would reduce the flow of blood into the tumor, causing it to shrink or wither away over time. Unfortunately, that approach was unsuccessful, else we’d be doing it today. A proponent of compression to treat bladder cancer (French surgeon Charles Le Clerc who lived 1644-1727) admitted that when this approach failed, the only other option was surgery.) Yet, in other treatments today (such as lymphadenopathy where the lower legs are swollen) compression garments are sometimes prescribed along with other treatments.
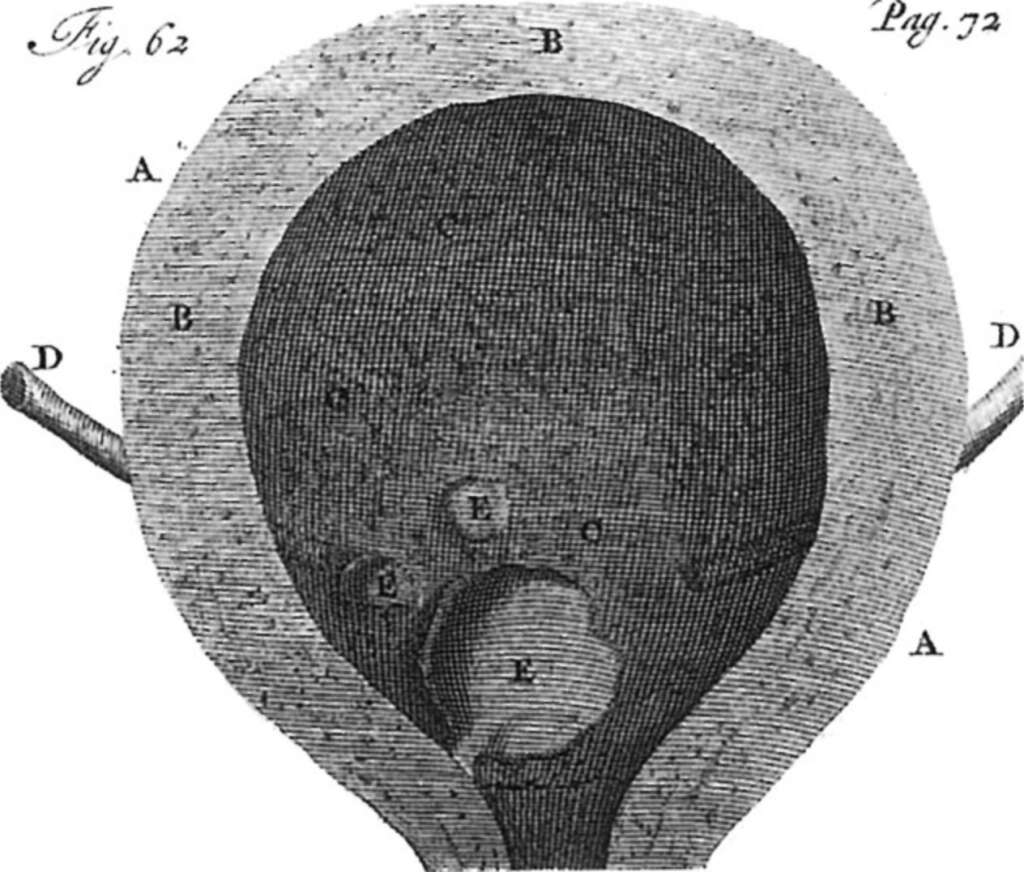
The first physician known to have recorded bladder cancer is generally considered to be Giovanni Maria Lancisi (1654 AD-1720 AD), an Italian physician, and anatomist.
Bladder tumor compliments of Fredericus Ruysch. Wiki Creative Commons.
While other historical records may reference conditions that could be interpreted as bladder cancer, it was finally Lancisi who specifically documented the disease in a medical context, making it one of the earliest formal records in medical literature. In his 1717 work titled “De Nocendis et Curandis Morbis,” Lancisi described the condition and its associated pathology. His observations contributed to the early understanding of what we now recognize as common bladder cancer. However, around the same time as Lancisi, a Dutch surgeon named Fredericus Ruysch (1638-1731) published a book called Observationum with a drawing of a papillary cancer tumor.
In one of my earlier posts I recall mentioning the relationship between certain industrial workers in England working with certain dyes the the proliferation of bladder cancer within that population. What I’ve included above takes us back in history another step or two
Now to urothelial cancer, which is what many of us have.
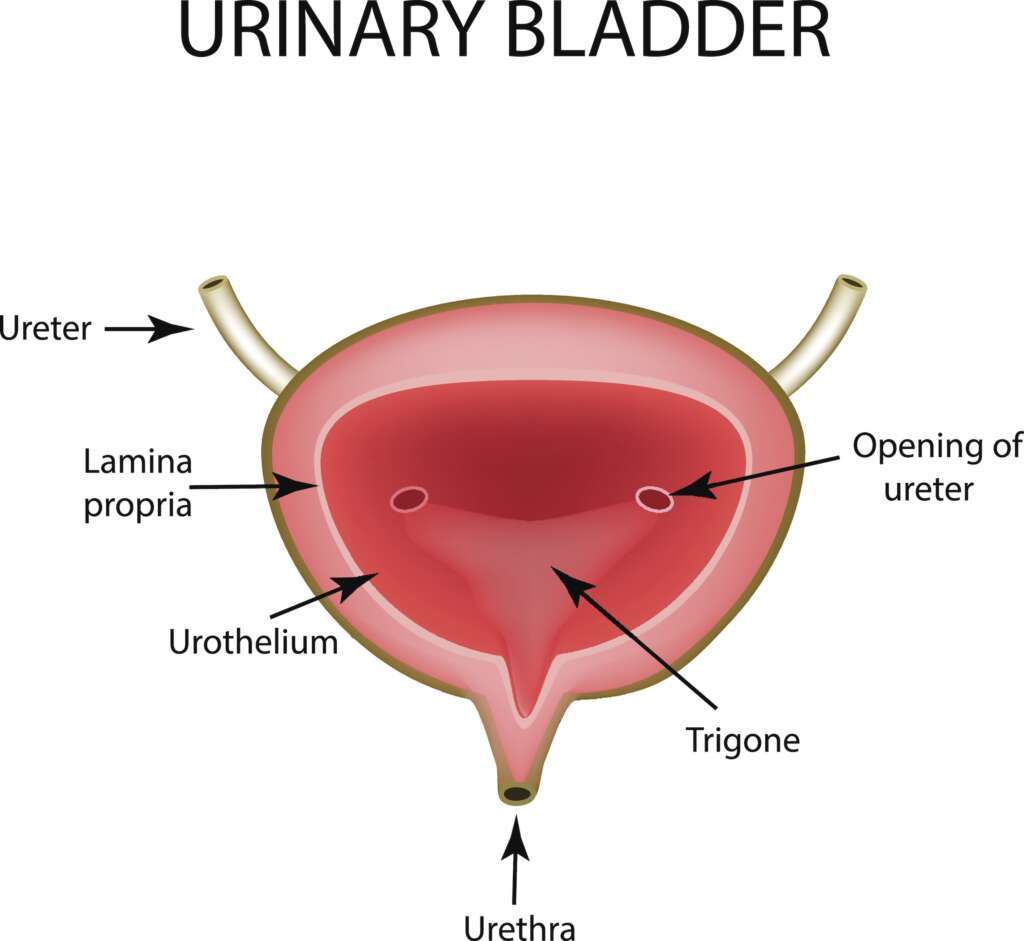
THE UROTHELIUM AND UROTHELIAL BLADDER CANCER
The urothelium is a specialized tissue layer that lines the urinary tract, including the bladder, ureters, renal pelvis, and urethra. Urothelial carcinoma, sometime known as transitional cell carcinoma, accounts for 80%-90% of all bladder cancers. What happens is the urothelial cells mutate over time, especially when exposed to carcinogens such as the wastes of tobacco consumption, exposure to defoliants or herbicides such as dioxin (Agent Orange) and other chemicals. These mutated cells are then malignant.
Anatomical structure of the Urinary bladder. Credit: Timoninalryna (iStock.)
In a TURBT, the cancerous growths embedded on the urothelium are scrapped off the lining and disposed of. This is why a TURBT is sometimes called a bladder scraping. If the cancerous cells are confined to the urothelium and have not invaded the muscle layer of the bladder, the bladder may be saved at the urologist’s discretion. What I mean by that is there is a professional organization in the U.S. called the American Urological Association (AUA), and a European counterpart. The AUA lists guidelines and treatment recommendations, which represent a consensus among American urologists in areas of cancer and the latest treatment modalities for treating bladder and prostate cancer. These recommendations form a sort of “best practice” set of guidelines, and while they are just recommendations, many urologists follow them because they are tried and tested and shown to be successful in terms of what can make a difference in a bladder patient’s outcomes. However, as far as I know, an experienced urologist is free to modify his or her approach to tailor the treatment in order to match the circumstances of the patient they are treating (this refers to the patient’s age, state of health, medical and surgical history, co-morbidities that the matient may have such as COPD, diabetes, chronic kidney disease, the patient’s wishes and so on.) In the near future I’ll explain how patients are “classified” or graded in terms of how robust they are. This metric is used in evaluating the general health of a patient who is being considered for surgery or some other strenuous regimen.
Incidentially, and to close the loop on the urothelium, the area from which the cancerous tumor is scrapped forms a scar tissue, but the urothelium can regenerate over time.
You might wonder what the urothelium does, why you have one. The Cleveland Clinic describes the function of the urothelium in an easy-to-understand way. They say that your urothelium:
Protects the rest of your body — like your blood vessels and muscles — from pee (which is acidic and could cause damage).
Prevents infections from pathogens (germs), like bacteria that cause urinary tract infections (UTIs.)
Helps transmit messages about what’s happening in your bladder to your nervous system — for instance, letting you know your bladder’s full and you need to pee.
Regulates the levels of water, salts and other substances in your pee.
Expands and contracts to enable your bladder tohold varying amounts of pee.
Later this month when my next pathology report comes back, I’ll go over what to look for on a cytology report and how to understand the report.
JANUARY 13, 2025 (M)
In two weeks, I have my sixth cystoscopy. I have had both high grade and low grade bladder cancer since January 2023. The low grade urothelial cancer has a good prognosis in terms of the odds of recurrence and life expectancy. High grade bladder cancer is more problematic, and it is more likely to return. So, I approach each cystoscopy mainly with a sense of optimism, but also prepared for that “Uh-oh” moment. All-in-all, cystoscopies are easier for me to deal with than my monthly chemotherapy treatments. There is less discomfort with the scope going through the urethra to the bladder vis-à-vis the subjective experience of a catheter. And, the procedure is usually less than fifteen minutes long.
JANUARY 5, 2025 (SU)
So, chemo went okay on Friday. Four employees at the clinic out sick from the Norovirus or some other bug, so it took a bit to find someone to catheterize me. Treatment went okay, except some Gemcidibine leaked out of the catheter (second time in the last few months.) I needed a Azolid tablet when I got home because it was too painful to urinate. No real restrictions on my activity or abilities after each treatment, though at 75 you never refuse the opportunity ot take a power nap in the afternoon. I wonder whether patients like me “wear down” over time or if it’s just a touch of depression I’m feeling? I was “gung ho” and ready for anything when I was first diagnosed. Two years later, treatment sort of wears you down, but Hey! I’m alive and otherwise healthy. I can’t complain. My next cystoscope is in two weeks.
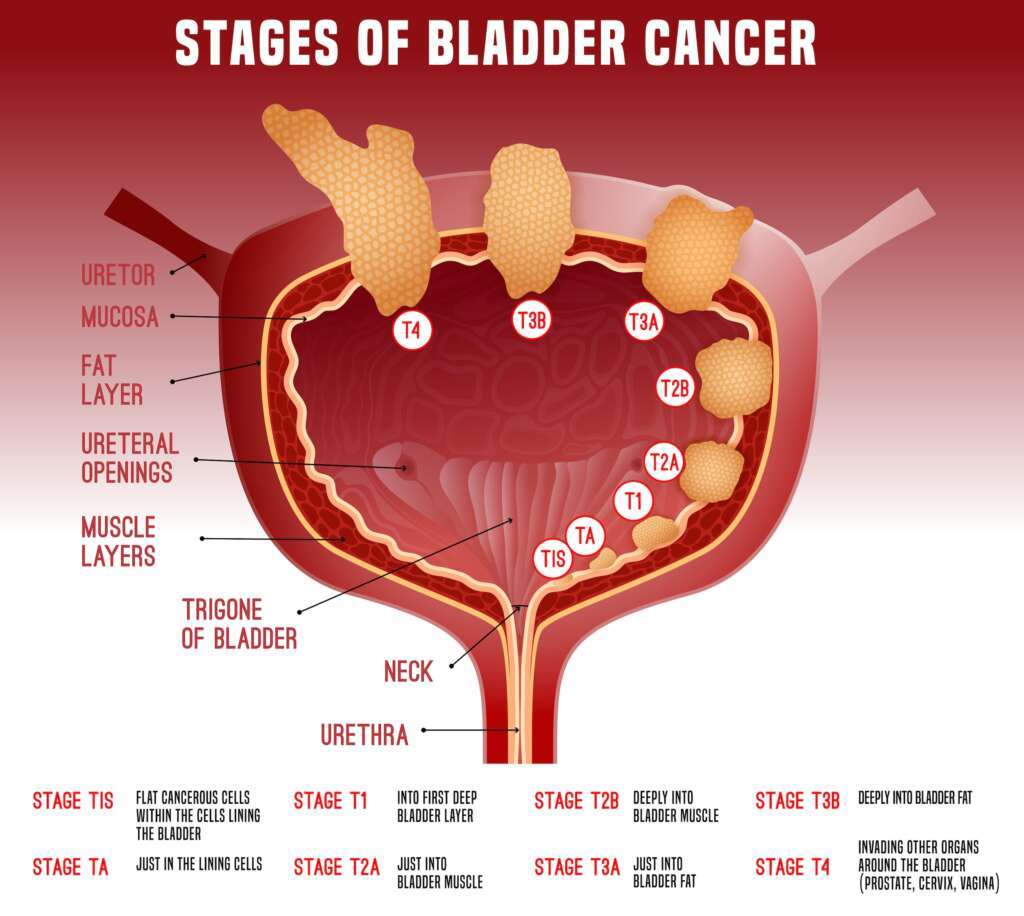
I have more and more people new to bladder cancer reading my posts. So, I found a usedful illustration that I’d like to add here (below), rather than try to revise an earlier post from February 2023. Click on the CT scanner image to start reading my journey with bladder cancer.
Stages of Bladder Cancer: Illustration credit: Anna Bergbauer (iStock.)
JANUARY 1, 2025 (W)
I wanted to accomplish several things with this entry. First and foremost, I wanted to wish the ~500 people who have read this thread a very Happy New Year. Even if the future looks bleak because of a prognosis, we can sometimes find reasons to be thankful. I am thankful that my cancer was caught before it spread elsewhere beyond my bladder, and that I still have my bladder. When I have my next chemotherapy treatment this Friday, I am thankful it will likely not make me really ill, like many who get BCG become ill, commonly from the immunological response of the tuberculosis being introduced into their bladder. This particular strain of tuberculosis (mycobacterium bovis) is an attenuated (i.e., weakened) form of TB that is found in cows. The treatment occasionally (but rarely) causes a TB infection in the person’s lungs or other complications elsewhere in the body. So, while a flu-like response to BCG may be the norm, a bladder cancer patient on BCG should always let their urologist/oncologist know how they are feeling.
I’m also thankful that in almost two years, my high grade cancer has not returned as far as I know, and that I have a wonderful physician and care team, a loving and totally supportive spouse, family and friends and so on.
I’m also thankful that I am not a physician, lol. This is a coy way of reminding the readers not to take what I write as the gospel. I do get involved in academic research, I’m fairly familiar with the professional literature, I’ve worked post-op on patients who have had their prostates removed or who have had other genitourinary conditions, but I am not a trained and licensed physician, and that is a big difference. If you read something that I write that seems interesting to you or is somehow “different” than what you’ve been told, always check with your physician before accepting the comments from a layperson (like me.)
So, there are two topics I want to blog about today. The first has to do with women who get bladder cancer and the second has to do with sex after a bladder cancer diagnosis in a male. Both topics are becoming increasingly important as younger and younger people are diagnosed with bladder cancer. In fact, younger people (i.e., folks in their twenties, thirties and forties) are contracting other forms of cancer not usually encountered until middle age or older as well as bladder cancer.
Bladder cancer in men is three to four times more common than in women. However, when the typical woman with bladder cancer is actually told she has bladder cancer, it is much further along than when an average male gets the formal diagnosis. So, all other things being equal, a woman with the diagnosis has a more problematic road ahead of her because the cancer of often more advanced. A fairly recent article “Gender Discrepancies in Bladder Cancer: Potential Explanations” by Pravin Viswambaram and Dickon Hayne says it all:
“The incidence of urothelial carcinoma of the bladder (UCB) is 3-4 times higher in men than women. However, women are more likely to be diagnosed with advanced disease. Women have a higher stage-for-stage mortality compared to men, and their greatest risk of death appears to be within the first 2 years of diagnosis. Survival outcomes following radical cystectomy (RC) and radiotherapy are also poorer in women. Delays in diagnosis, differences in female anatomy, as well as poorer surgical outcomes post-RC appear to contribute significantly to the disparities noted between genders. Other factors such as exposure to risk factors, differential hormone signaling, and carcinogen breakdown may also have a role.”
What these authors are saying as I understand it is that there are numerous variables at work, some known and perhaps some yet to be discovered that cause differing outcomes between men and women with bladder cancer. What I am learning from women who are battling bladder cancer is that it often takes repeated trips to their primary care doctor with a complaint of blood in their urine or for pelvic pain before CT scans and other definitive tests are ordered. It was just over two weeks from my first urinalysis with blood present to my CT scan revealing bladder cancer. It was less than a month from my first urinalysis to my first TURBT (bladder scrapping.) That was entirely reasonable time-wise. Twice as long as a month might or might not be a problem, but that is a question for your doctor. But waiting for “months” can be the difference between catching the cancer when it is somewhat less advanced and requiring the removal of the bladder. Women say that the blood they report or which is observed in their urine is often dismissed as menstrual, and if pain is present, then it is thought to be a urinary tract infection or a kidney stone passing through. There is, in fact, some logic to this conservative approach. Doctors for several reasons always begin with the more common or obvious reason for the presentation. My point is that women (like men) need to be assertive about their health. If, after the first visit the problem persists, and supposing I were a woman for the sake of argument, I would say to my doctor: “You know, I’m fairly concerned here. I would feel much better if you would order some sort of CT, or MRI or cystoscopy. I have a family who loves me, small children who need me, etc.” Your physician may have to battle in-house patient accounting officers, financial compliance officers, insurance companies, etc. on a daily basis, so doctors today do not always have the final say. And, there is a patient advocate or ombudsman at your hospital that can sympathize with your point of view if you look them up. You never want to find yourself in an adversarial relationship with your doctor. The strategy is to be firm but always polite and friendly. There may be reasons that what you suggest is just not possible or useful. And then, there is always the option of a second opinion. This is a professional choice and no feelings should be hurt.
And while I’m talking about women and bladder cancer, more and more young people are getting bladder cancer. Many of them are women. One cause of bladder cancer relates to repeated urinary tract infections (UTI’s.) Because women are more prone to UTI’s than men for several reasons, it’s important for women to have their UTI’s promptly treated. Again, while I’m not a doctor, if a female of any age gets more than two or three UTI’s a year, I would think they might be better off visiting a urologist than just a PCP. Then, again, UTI’s can sometime cause irreparable kidney damage. So it’s important to stay on top of this.
The second issue I want to mention deals with coitus between a male with a history of bladder cancer and a female. The general consensus within the medical community seems to be that “Bladder cancer is not a sexually transmitted disease. A female cannot contract bladder cancer through sexual intercourse with a male who has bladder cancer” according to Pathway, a medical decisionmaking app for physcians. Part of the reason is that bladder cancer is caused through mutations in the bladder cells, themselves, and absent these cells in a healthy bladder, the cancer cannot proliferate. The only sexually-transmitted viruses with the potential for cancer are the human papillomavirus (HPV) and human immunodeficiency virus (HIV.) But again, verify this against professional medical advice. It may be embarrassing but there is no other way you can know for sure.
The Cancer Council of Victoria offers the following useful information:
Be assured that it is not possible for your partner to transmit cancer through intimate activities such as kissing or intercourse.
Sexual activity will not make cancer spread, nor will it make the cancer come back.
Chemotherapy drugs may stay in your partner’s body fluids for some days. Using condoms or other barrier methods for a week after treatment can protect you from any potential risk.
It will usually be safe to have sex after radiotherapy. If your partner is having external radiotherapy, they will not be radioactive once they return home. If your partner is having internal radiotherapy (brachytherapy or radioisotope therapy), you may need to take some precautions, such as avoiding sexual contact or using condoms or other barrier methods, particularly during pregnancy – your treatment team will be able to advise you.
If your partner is receiving immunotherapy for bladder cancer (Bacillus Calmette- Guérin, or BCG), ask their treatment team what precautions you need to take. You will usually have to avoid sex for 48 hours after each treatment, and then use condoms or other barrier methods during the rest of the treatment cycle and for six weeks after the final treatment.
p.s. For those who are curious, AI provided a detailed explanation below as far as why cancer cells from one person would not normally grow in another person. If anyone has a specific question about what follows, please feel free to leave a comment on this post and I’ll try to answer it.
Cancer cells are the result of mutations and abnormal cell growth that occur in an individual’s body. There are several reasons why cancer cells from one person cannot typically reproduce or thrive in another person:
Host Immune Response:One of the primary defenses against cancer is the immune system. When foreign cells, such as cancer cells from another individual, are introduced into a person’s body, the immune system often recognizes these cells as foreign proteins through a process called immune surveillance. This triggers an immune response that tries to eliminate the foreign cells.
Genetic Differences:Cancer cells contain mutations that are often specific to the individual from whom they originated. These genetic variations can affect how the immune system recognizes and reacts to the cells. Even if cancer cells from one person were transferred to another person, the genetic differences would generally prevent those cells from adapting effectively to their new environment.
Microenvironment and Support:Cancer cells thrive in a specific microenvironment that includes various factors such as growth factors, extracellular matrix components, and signaling molecules. Each individual has a unique physiological environment, which means that cancer cells may not receive the necessary signals and support to survive and proliferate in a different body.
Tumor Heterogeneity:Tumors are often composed of a heterogeneous population of cells with various genetic and phenotypic traits. The specific adaptations that allow cancer cells to grow in one individual may not be suitable for survival in a different individual’s body.
Transplantation Challenges: Even in cases like organ transplants, where cells from one individual are introduced into another (e.g., bone marrow transplants), there is a high risk of rejection due to the immune response. Cancer cells would face even greater challenges in a foreign host due to their atypical characteristics. There are rare exceptions, such as in cases involving xenotransplantation (the transplantation of cells or tissues from one species to another), or in specific situations involving immunocompromised individuals (where the immune system is weakened), but these are not typical and come with significant risks and complications. Overall, the unique combination of immune rejection, genetic factors, and microenvironmental conditions makes it highly unlikely for cancer cells from one person to reproduce in another.
I hope everyone has a very Happy New Year!
OCTOBER 23, 2024 (M)
The pathology on my bladder washing (where normal saline or some other sterile solution is used to irrigate the bladder and then retrieve the solution which is sent to the lab for analysis came back this morning. It read:
Without reading into this more than what is reasonable, I think this is the best cytology report I’ve had in a year. In the past, my random cells were identified as benign but abnormal or benign but reactive. This left the door open a crack for a future diagnosis of urothelial cancer. I can’t consider myself “cured” at the moment, Usually, a cancer patient has a burden of going for five years without a return of their cancer to be considered “cured,” and a year from now I will barely be at the half way point. And I’ve known some oncologists who don’t have the word “cured” in their vocabulary, even.
Cancer patients learn to live for the day, which is what I’m doing at the moment.
OCTOBER 9, 2024 (W)
Scheduled for a quarterly cystoscopy this afternoon. Hopefully there will be a good report. Back in a bit . . . Stay tuned.
My urologist-oncologist is very happy after the procedure. Bladder looks the best it has all year. God be praised!
“FINDINGS:
The anterior urethra appeared normal.
The prostatic urethra appeared moderate
The ureteral orifices were normal.
Bladder neck was normal
The bladder appeared normal.
There were no mucosal lesions suspicious for neoplasm. There was a scar on right bladder wall with minimal flat errythema
There were Grade 2 trabeculations. Bladder diverticuli were noted at the dome
There were no foreign bodies.
Cytology:Yes
Biopsy: No Location: not applicable
Culture: No
Cystoscope was removed and patient tolerated procedure well.
ASSESSMENT:
High risk non-muscle invasive bladder cancer (Hg Ta>3cm)
– Participating in clinical trial randomized to gem/doce
– annual imaging due 7/2025
– continue with q3 month cystoscopy
-continue with two years maintenance”
September 25, 2024 (W)
So, I had chemotherapy today and it went well. I learned that I will receive chemotherapy monthly at least until next June (2025), which will make it twenty-eight months of chemo since my bladder tumor removal. Since I started chemo, I was part of a study that compared patients getting BCG to those getting chemotherapy (Gemdoce.) However, I understand in my region of upstate NY, BCG is no longer available, so I’m not sure what that means as far as the study is concerned. When I began post-TURBT treatment, I received each of the two drugs consecutively, and had them remain in my bladder for two hours each. A year ago, that time was reduced to one hour per application per medication. I’ve read of cancer centers in other parts of the country that have cut the BCG dose strength in half to deal with the shortage of BCG. Cancer patients such as I cannot help but wonder whether the efficacy of these changes might compromise care. Merck, the only producer of BCG in the U.S. and for other countries as well at the moment estimates that it’s new manufacturing facility won’t be online before 2026, so this is not a good time to have bladder cancer if you are pinning your hopes of recovery on BCG. Fortunately, Gemdoce is essentially as efficacious as BCG all things beging equal.
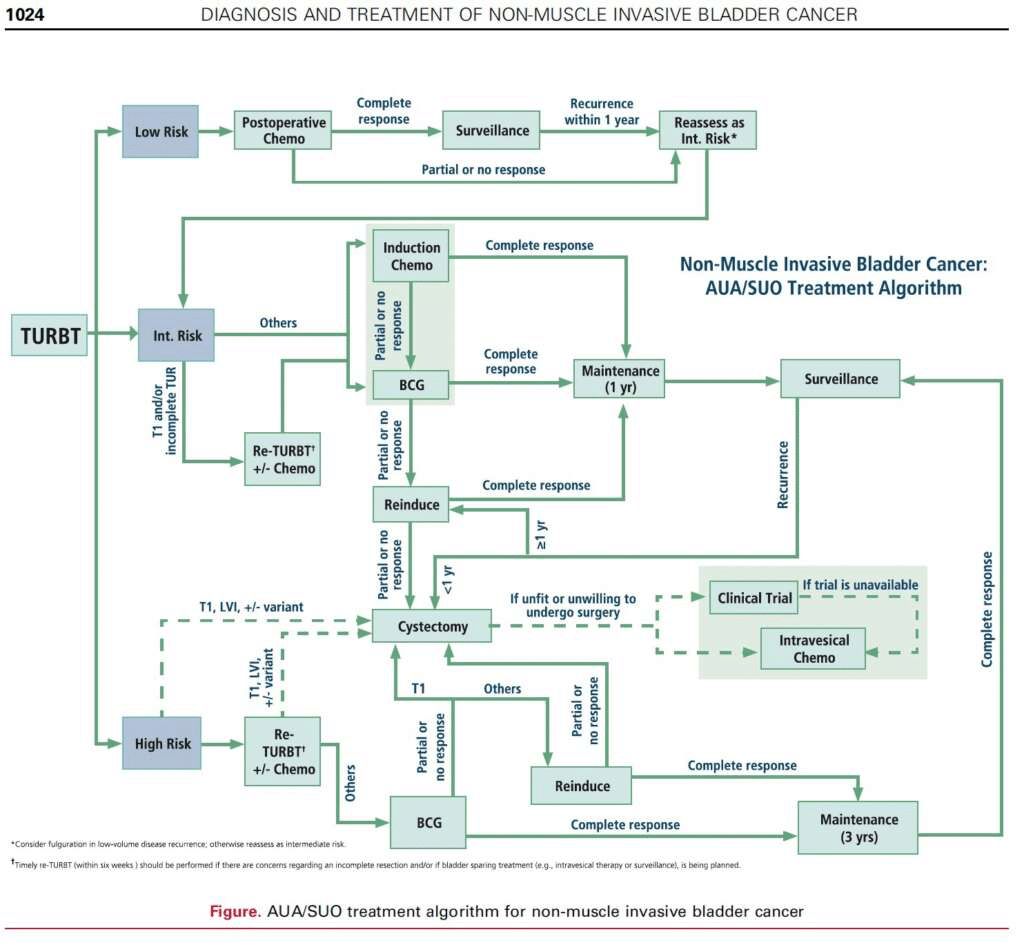
I’ve included the algorythm that many urologists use to decide how to plan a patient’s care after their TURBT and response to relapses, etc. This chart is provided by the AUA/SUO.
July 30, 2024 (Tuesday)
My cytology report is in:
“Benign. Reactive urothelial cells.“
This analysis is based on draining the bladder contents after the cystoscopy and analyzing a random sample of the free floating cells (including any that are suspicious in appearance I would hope.) The report is good (benign.) The next few years for someone with high grade bladder cancer is a bit fuzzy though. For example, what are “reactive urothelial cells?” According to the prestigious journal Nature,
Reactive urothelial cells show mild abnormalities that are shared by low-grade neoplastic cells and require considerable screening time from pathologists and cytologists. The presence of significant abnormalities warrants a diagnosis of atypias suspicious for malignancy.”
Sigmund Freud. Credit: Max Halberstadt, Public domain, via Wikimedia Commons.
So, normal cells do not transition to cancer cells overnight. In the absence of cancer, there is a transition from benign to malignant caused over many generations of cells. The lifespan of a normal urothelial cell which lines the inside of the bladder is 40-41 weeks in length. On the other hand, if there are a few intact cancer cells lurking somewhere out of sight, all they need to do is reproduce, and that process is quite rapid. Reactive urothelian cells are abnormal cells. Mine do not presently meet the criteria to be called cancer. However, those cells of mine which were examined under a microscope show the sort of interim changes (mutations) that are seen in cancer cells. On the other hand, they may never transition into cancer. As Freud said, “Sometimes a cigar is just a cigar.”
Tomorrow I have a chemo treatment. Truth be told, I get weary somewhat with the process, although what I am experience is absolutely nothing compared to what many cancer patients go through. I’ve seen and treated many cancer patients and I fully understand that if cancer is my major health risk in this decade of my life, then God has blessed me with bladder cancer rather than the horror of breast, lung, brain, colon, pancreatic, bone or some other form of cancer.
Still waiting for the biopsy results. That usually takes a week or more, especially if there is a peer review or referee process involved.
July 26, 2024 (Friday)
I saw my urologist/oncologist on Wednesday for my quarterly cystoscopy. On these occasions, they insert a flexible catheter that has the utility and variation of a Swiss army knife. In other words, it can allow her to scope my bladder, biopsy my bladder, cauterize my bladder, flush it out with a saline solution and capture the residue. For all I know, it may provide her with the time, temperature and the weather forecast. Here is an extract from her notes:
FINDINGS: The anterior urethra appeared: Normal. The prostatic urethra appeared: Normal . The median lobe was Present. Small. The ureteral orifices were Normal. Bladder neck was Normal. The bladder appeared Abnormal There were areas of erythema noted at the posterior bladder and right lateral wall. Area of erythema at posterior bladder was biopsied.
Trabeculations noted: Yes
Diverticuli noted: Yes. Small. Noted near dome, explored with normal appearing mucosa. There were no foreign bodies. Cytology sent: Yes Biopsy performed: Yes Urine culture: No
Cystoscope was removed and patient tolerated procedure well.
Assessment/Plan:
#High risk non-muscle invasive bladder cancer (Hg Ta>3cm)
– Cysto today much improved
The areas with erythema are areas that appear to be irritated of inflammed. While inflammation in other areas of a body (such as a swollen wrist or a person’s gums) can be painful, fortunately, I am not experiencing any discomfort. There are several causes of such red spots, though the most common cause is an inflammatory process, such as irritation to the urothelial layer of the bladder by my chemotherapy drugs which I receive once a month. However, “. . . the rate of diagnosis of CIS in a de novo red patch is 8%. . .,” so it is prudent to biopsy any red patches noted, and my urologist did. The findings of this biopsy and the analysis of my bladder fluid will provide the finishing brush strokes on the portrait on my bladder health at the moment.
Bladder trabeculations refer to areas of the bladder which are “thicker” than other areas. In places of the bladder where trabeculations are noted, there is a loss of elasticity of the bladder, which makes it difficult to empty one’s bladder normally. These trabeculations are something I am cognizant of, and I must “bear down” several times to empty my bladder after the urge to urinate passes.
DIverticuli refers to small pouches or cul de sacs in the wall of the bladder (or other organs of the body, most notably the colon which are the cause of diverticulosis. These pouches (whereever they are found in the body) are capable of producing irritation and can ofter become malignant. So, a good oncologist pays close attention to any diverticuli noted.
So, with the caveat that the cytology on the bladder fluid and the pathology on the biopsied tissue still remain to be analyzed, my bladder appears to be “much improved.” For this I am grateful.
June 26, 2024 (Wednesday)
Had my monthly chemotherapy today. It went really smoothly all around. I’ve been reading about more and more bladder cancer patients getting BCG, or the tuberculosis variant. Even giving them partial doses of BCG to make more bacteria available to other patients is giving the patients significant pain after the first 4-5 doses. BCG is different than chemotheraty because it actually produces an immune response, so your body may well develop flu-like symptoms.
For years, BCG was the gold standard for bladder cancer treatment, but there have since been chronic shortages. Here is a talking point paper I did a year ago:
411 on Bacille Calmette-Guérin (BCG)
TIME LINE
1920 Bacille Calmette-Guérin: First strain produced after 231 iterations combining bovine bile and Mycobacterium bovis (bovine TB) from a cow with tuberculous mastitis (p. 3).
1929 Biologist Raymond Pearl doing post-mortem studies at Johns Hopkins “reported a lower frequency of cancer in patients with tuberculosis.” (p. 3). “In other words, active tuberculous lesions occurred more than twice as frequently in the controls as in the malignant group. Healed tuberculous lesions occurred with equal frequency in both groups. In each decade of age and in each sex and race the percentage of persons showing active tuberculous lesions was higher in the control than in the cancer group”. Cancer and Tuberculosis, Raymond Pearl. American Journal of Hygiene, 1929 Vol.9 pp.97-159 ref.135.That was the first anecdotal link between cancer and TB.
1976 Following success in the use of BCG which was introduced via intravesical route into the bladders of guinea pigs with cancer of the urothelium, the first clinical trial of intravesical BCG was conducted. A. Morales, et al. were able to demonstrate a “remarkable decrease in the rates of recurrence of superficial bladder cancer in nine patients”. A randomized prospective trial by Lamm et al. in 1980 confirmed these earlier observations. Since this time, it has been shown that BCG, when used, has an inferred benefit to those with superficial bladder cancer in terms of decreased recurrence rate and increased time to recurrence. (p.3)
STRAINS
There are several different strains of BCG available, with the Tice strain, the RIVM strain and the Connaught strain being the most common (p.3). However, there seems to be no consensus on the relative efficacy of one strain vis-à-vis another.
MECHANISM OF ACTION
“The exact mechanism of action of intravesical BCG is not completely understood” (p.6). However, BMJ Postgraduate Medical Journal attached discusses several contending hypotheses (See attach.)
WHY IS THERE A BCG SHORTAGE?
“For a long time, there were 2 manufacturers of BCG; (one) in the United States and (one_ Canada. In 2012, Sanofi Pasteur in Canada, which manufactured the Connaught strain, went offline because of some inconsistencies in their manufacturing.”[1]
Two years later, Sanofi has the BCG Toronto laboratory cleared to make the drug. But now they have decided to end production, most likely because the profits of manufacturing the strain did not compensate for the costs of retooling of their plant.
Meanwhile, the Merck plant which manufactures the vaccine is having contamination problems of its own which require intermittent shutdowns for contamination of the product.
Woke up around 4:10 a.m. I wanted to sleep some more, but I try to be a little tired for chemotherapy because it seems to take the “edge” off some of the more unpleasant aspects of the procedure. My treatment is at 10:45 this a.m. Once again, I thank God for sparing me from the sort of side effects that many cancer patients have with their therapy. I’ve been reading some of the accounts of other bladder cancer patients who have been receiving Bacillus Calmette-Guerin (BCG.) BCG is a variant of the bacteria Mycobacterium tuberculosis which causes tuberculosis, though in this case, bladder cancer patients do not actually get TB because the bacterial strain is either attenuated (weakened) or has been genetically modified in some way. About a century ago (1929), Biologist Raymond Pearl doing post-mortem studies at Johns Hopkins “reported a lower frequency of cancer in patients with tuberculosis” which seemed odd to him:
In other words, active tuberculous lesions occurred more than twice as frequently in the controls as in the malignant group. Healed tuberculous lesions occurred with equal frequency in both groups. In each decade of age and in each sex and race the percentage of persons showing active tuberculous lesions was higher in the control than in the cancer group”.
This suggested to Peal that the TB bacteria was able to “shut down” or impede the growth of cancer.
Therefore, BCG is not chemotherapy, but rather immunotherapy. The personal accounts I’m reading from patients receiving BCG therapy makes glad in some way that I was not selected to be in the BCG group of the study I’m in. All things being equal, it seems like the data is showing that in cases of nonmuscular invasive bladder cancer, certain chemotherapeutic drugs are as effective as BCG. Many–but not all–BCG patients are noting muscle soreness, low grade fevers, and generally feeling unwell for a day or two after treatment. This suggests an immune response to the bacteria and this indicates the treatment is working. Patients with a lack of flu-like symptoms may not be able to develop this response in their bodies and the bacteria in their cases may not be working as hoped against their cancer. But it would take procedures such as a cystoscope, perhaps a CT scan, etc. for a urologist/oncologist to make that determination.
I’ll be back later today after my treatment.
3:30 p.m. So, my treatment went very well today. In fact, it was probably the best one yet out eighteen treatments altogether in terms of a pain-free catherization. At the moment, I’m trying to flush out the second medication from my bladder. It is highly toxic, and the solution is highly flammable.
May 30, 2024 (Thursday)
I have a chemotherapy treatment tomorrow. I have a little apprehension every time an additional treatment approaches. There is nothing that can go wrong other than a urinary tract infection, but the employees at the urology clinic have generally good technique, and the nurse practitioner is a friend of Deena and me.
Tonight I have to take the first of four sodium bicarbonate (HCO3) tablets which shift my pH in anticipation of the treatment. I’m not sure if it is to reduce some unpleasant irritation from the chemotherapeutic agents or if the HCO3 potentiates the drugs.
I have been spending a bit of time on some of the social media forums that have bladder cancer subgroups. There are new people each week between the ages of 25-35 that report they have been diagnosed with bladder cancer. These are often people with young children who never thought anything like this might happen to them, especially at that age. So, I’ve been trying to encourage them the best I can. Other people are having really rough times with unrelenting bladder spasms or blowback from BCG. BCG is a weakened tuberculosis bacillus that evokes an immune response in the body of the patient. That usually accounts for their aches and pains. Others have their first bladder surgery and they don’t know what to expect or what questions they should ask of their doctor.
May 5, 2024 (Sunday)
Received a surprise today. A missing piece of the puzzle arrived on the patient portal. There were three biopsies done of different areas of my bladder plus a bladder washing which is always performed after a cystoscopy. The washing consists of scraps of organic debris, urothelial cells and perhaps malignant cells as well. The report finding said: “Bladder, washing: Benign. Inflammation and reactive urothelial cells.”
-More to follow-
May 1, 2024 (Wednesday)
My pathology from last Wednesday posted this afternoon with the conclusion: “Acute cystitis with mild atypia, favor reactive.” The term “acute” means “sudden” or “severe” in the context of health science. The term “cystitis” refers to an inflammation of the bladder. “Atypia” refers to something that is unusual, not normal. There are two categories in a sense here; Atypical favoring reactive (urothelial cells) and atypical favoring neoplasm. In my case, it was the former. And, as is typically the case, the pathologist’s conclusion was peer-reviewed.
What causes cystitis or inflammation of the bladder? Probably the most common cause is an infection. But in the absence of an infection, it can be drug-related and be caused by my chemotherapy for example. It can come from certain chemicals such as buddle bath solutions. It can be caused by radiation applied to the pelvic area. Cyctitis can also be caused by kidney stones or indwelling catheters. Finally, cystitis can be found alongside certain conditions such as diabetes or an enlarged prostate.
So, for now I’m doing good. I had chemotherapy today and in a few days Deena, her sister Debbie and I will be headed for a vacation in Maine.
Thanks be to God.
April 30 2024 (Tuesday)
A week since the biopsies and bladder wash was submitted to pathology and no word yet. No surprize at the processing time, but our imaginations have been working overtime and we’re prepared for a disappointing report. Erythemas (red, inflamed areas) of the urothelium or inner lining of the bladder as noted in my cystoscopies of Jaunary and of late April can be a common sign of CIS (carcinoma in situ.) In situ in the context of cancer refers to cancer cells what have not yet spread. The high grade classification of my cancer means that the proliferation of malignant cells into other structures of the bladder is just a matter of time. So, Deena and I are both feeling the stress. We see the possibility of another TURBT procedure in the near future at least, and a removal of the bladder, prostate and a portion of the illeum (distal small bowel) at worse. But we just don’t know until the cytology/pathology report arrives.
My urologist wrote that she wants my next chemotherapy treatment in late May, but someone scheduled me for chemo tomorrow. We’ll have to get that clarified when I report to the clinic in case my doctor does not want me to have chemotherapy for the time being. With a trip out-of-state planned for this coming weekend, we also wonder whether I’ll leave the clinic tomorrow with a bladder infection following treatment (assuming I receive treatment tomorrow.) This has only hapened once in over a dozen treatments, so the odds are fairly remote that it will happen again.
Definitely, more to follow.
April 27, 2024 (Saturday)
Waiting is the hardest part as any patient will tell you. Until you receive your cytology/pathology report, you are neither well or unwell absent any symptoms. As of today, there is no word. It will probably be midweek around May 1st before anything comes in.
I had a strange dream last night. I was working in a metropolitan area either in the Mayor’s office or the Emergency Services office and there was a nuclear even in the city. I’d don’t recall whether it was an accident or an attack from some foe. My surpervisor directed me to reconnoiter(i.e., scout) the damage and report back. I did, trying to avoid areas that I though might have dangerous radiation levels lest I become contaminated and poisoned by gamma particles as the unfortunate people of Hiroshoma or Chernobyl were.
Was that just a random dream, or was my subconscious suggesting or warning me that at some point in the future my cancer treatments mught switch from chermical chemotherapy to radiotherapy?
April 24, 2024 (Wednesday)
I had a quarterly cystoscopy today, and it seems to be the most problematic of the four that I’ve had to date. I could not clearly see the monitor, but I did note half a dozen white pearl-like circles which seemed unusual. There were areas of inflammation which my urologist said were possibly from my chemo, even though it’s been six weeks since my last treatment. My doctor performed a tour de force sweep of my bladder while frowning. She navigated back to certain areas mentioning that she would perform a bladder washing and then threw in several biopsies as well. The biopsies weren’t bad, but the cauterization stung a mite. Things were pretty quiet up until that point with Deena and I and my physician, a resident and a nurse standing quietly in the room, but suddenly it seemed like a flash mob of other assistants appeared. I remarked to the doctor that I would have brought our golden retriever Molly along if I knew there was going to be a party. Now, for the waiting. . .
April 1, 2024 (Monday)
Today, my urological oncologist phoned me unexpectedly. Over then next twelve-to-fifteen minutes, she did a case review of sorts while Deena and I listened. Most of the several nodules on my lungs are only 2 mm in diameter. The largest nodule is 4 mm, which is slighly smaller than a standard pencil eraser. A nodule that is 2 mm is the size of the black dot below.
My doctor told us that at present, the nodules were too small for a PET Scan, and that even in bladder cancer patients, most pulmonary modules were benign. She also mentioned that we likely know otherwise healthy people who have similar nodules but who are not aware of them. She then spoke to the fact that a CT takes photos of small slices of the lungs, 2mm or less in “thickness” and that small nodules are not always apparent.
She also seemed to indicate that a repeat urinalysis was not necessary unless I had signs/symptoms of a urinary tract infection. As far as whether the 1+ blood was suggestive on cancer, she did not seem concerned unless I had visible bleeding.
March 29, 2024 (Friday)
Earlier this week, Deena took me to see a nurse practitioner at our practice as our PCP was booked. My complaint was an unusual, intermittent pain in my left clavicle (collarbone.) I had not injured the area and in the past I would have balked and chalked it off as just aging. It has bothered me on and off for the past month to six weeks, and I hoped the NP would have it x-rayed as cancer does metastasize to the collarbone, especially if it is in the neighborhood. Admittedly, this was a stretch, but as I mentioned to the NP, the odds of it being early metastasis were greater than zero, even if only two or three percent. And, with six Agent Orange diseases or disorders presumably from my year in Vietnam, what is one more? It could be an occult fracture from multiple myeloma, though there was no point tenderness around the bone, other evidense of myeloma and this thought did not occur to me at the time. Nor do I have any reason to suspect myeloma. The NP took an EKG which was a good precaution and it was read as normal, though the quality of the EKG was not the best I’ve seen. The x-ray of my collarbone was normal (thankfully.)
Yellow flag danger signal for motor sport. Credit fabioderby (Adobe.)
Today, I had chemotherapy with a new nurse. It went well, though because of a recent change in procedures, they had not intended to run a urinalysis before administering the chemotherapy drugs. Deena was persistently insistent that they do, and when the results popped up on my phone thirty minutes later, it noted that I had 1+ blood in my urine. Not the end of the world. It might have come from some minor capillary bleeding associated with placing the catheter, but if you compare getting catheterized and having a recent history of bladder cancer to a NASCAR race, it would be the equivalent of a yellow flag. It would not be prudent to ignore the test until blood was frankly visible to me. I won’t make that same mistake twice!
My experience from working in hospitals and personally being the advocate of a critically ill spouse who succumbed to her illnesses before I met Deena, tells me that you as the caregiver need to pay a vigilant role as the advocate for your spouse, parent, child or whomever is seriously ill in your family. You need to be assertive! On the other hand, you don’t want your care team to cringe whenever they receive a message from you. Yet, a (mercifully) few patients do fall through the cracks from time-to-time. They get ill from hospital-acquired infections or receive the wrong dose or wrong medication from the pharmcist. Many, many years ago, I almost administered a potentially lethal dose of digoxin to a cardiac patient because I overlooked the decimal point in the dose. Fortunately for the patient, the charge nurse was at the medicine station wondering who ran off with all of her dig.
A recptionist in training may fail to convey an urgent message to the physician. Sometimes, because of supply shortages, patients do not receive the drug of choice for their illness, or a pre-certification for an expensive procedure is not forthcoming from the insurance carrier. Wait times in emergency rooms which used to run three-to-four hours after triage are now sometimes four times that. Yesterday’s chemo treatment was changed three different times in as many days, as far as time or place goes. Hospitals and clinics are short staffed under ideal conditions, front line doctors and nurses are exhausted, and so on.
Quite a few doctors discourage their patients from researching their medical problems online. However, if you get your information from a credible source (e.g., the Mayo Clinic, Cleveland Clinic, Johns Hopkins, or the professional organizations such as the Bladder Cancer Advocacy Network, Altzheimer’s Foundation, etc.), I think you are better off for having done so.
As my chemo treatments go, it was one of the better ones. Hopefully, I’ll be able to get a repeat urinalysis this coming week to rule out a bleeding issue without having to pester my urologist yet again.
March 20, 2024 (Wednesday)
The last six weeks have been uneventful. On February 18, I started Ozempic®. My A1C (glucose) value has slowly crept up over the past year, but it was still pretty good for a Type II diabetic. However, being a diabetic gave me medical drug coverageand a reason to access Ozempic, and I hope to lose forty pounds (it works like Wegovy®), which would might give me some advantage in any future surgeries or cardiac event. I’m currently losing a tab over a pound a week, and I’m still on a low, introductory dose.
My end of February chemotherapy treatment went really well–both the catheterization and the immediate recovery.
And now, the news
That brings us up to this week. In January 2023, I had a CT scan that noted the bladder cancer. It also noted a small “nodule” near the base of my right lung. The radiologist’s recommendation was for me to have another CT scan later last spring, and I did. There was no change in the nodule by then. My oncologist wanted me to have a brand, new CT work-up this past January on the first anniversary of my diagnosis, and she wanted the nodule to be revisited as well. However, there was no order to scan my lungs in January, so she had to order another CT for my lungs (and she threw in my bladder again as well. I think that was perhaps because she wanted to see if there was any correlation to that “pink spot” I described below.) Here is what they found:
There were no findings “suspicious for metastatic disease.”
The radiologist noted a “possible subtle asymmetry near the superior margin of the original bladder mass.” To me, this suggests that something may be displacing the bladder wall, producing a barely noticeable bulge, but I have no idea if I’m correct..
“There was a “mild thickening/trabeculation of the wall . . .slightly more pronounced at the right superior bladder wall, positioned slightly above the original right bladder mass. Cystoscopic correlation/follow-up” was suggested.
The word “trabeculation” refers to a loss of elasticity. The bladder is like a balloon, which stretches as it fills. Trabeculation occurs when there are obstructions to the outflow of urine from the bladder (e.g., kidney stones, enlarged prostates in men) trauma (and tumors.)
There was an innocent-appearing remark on the report under the category lung bases which read “Please see separately dictated chest CT exam.” For a day and one half, there was not a second report, but late yesterday afternoon it popped up on the portal.
The second report began with good news: “There are no pathologically enlarged thoracic lymph nodes” and “there is no pulmonary mass, consolidation, or ground-glass attenuation.” But then it went on: “Small solid, noncalcified pulmonary nodules measuring approximately 4 mm in the middle lobe lateral segment and 2-3 millimeters posteriorly in the left lower lobe are noted. . .” before concluding “above-described small lung nodules may very well be benign but are indeterminate as small metastases could demonstrate appearance in this patient with a reported history of bladder cancer. As such, these nodules should be reevaluated in 3 months follow-up CT scan of the chest.”
What might cause these tiny lesions. The thickening of my bronchial walls noted elsewhere on the scan could be caused by infections, which could also scar the lungs in a way that the radiologist noted. But bladder cancer that has spread to the lungs appears the exact same way. So he seems to be saying “If this patient were a normal guy (and I can assure you that he isn’t), then these nodules would machts nichts (i.e., make no difference.) But since he’s had bladder cancer, it might have spread (and now there is not just one nodule in one lung, but several in both lungs.)
In that case, how did those critters get loose? And how did they get to the lungs? The lungs are a long way from the nether regions of the pelvis. My cancer seemed to be confined to the inner lining of the bladder, so there was little immediate concern that it might metastasize elsewhere. Usually, cancer spreads physically to an adjoining organ, or via the lymphatic system or the bloodstream. But there was never any indication of swollen lymph nodes. As far as the blood stream goes, who knows?
So, Deena and I expect that my oncologist will order a PET scan (Positron Emission Tomography.) In a PET scan, radioactive glucose is injected in the patient’s body. A cancer cell seems to have “sweet tooth” and the machine can trace where the glucose winds up, targeting specific areas.
So, how is this impacting Deena and I?
Deena and I have similar and different thoughts about this. We both hope for the best, but prepare for the worst. She has been widowed before and the last thing I want is to make her a widow for a second time. Nothing like this was on the radar when we first met six years ago.
Sometimes I think of this as a particular place in the road of life. Like, the Slough of Despond in Bunyan’s book “Pilgrim’s Progress.” Here, the protagonist must travel through a land from Point A to Point B (life to death) and the road passes through places such as “Vanity Fair,” or “The Doubting Castle.” Bunyan describes the Slough as:
. . . there ariseth in his soul many fears, and doubts, and discouraging apprehensions, which all of them get together, and settle in this place; and this is the reason of the badness of this ground.“
AI image credit: Nilima (Adobe.)
Or, there is a famous saying that life is a “vale of tears” through which we go. Based on Psalm 84:6, it testifies to the Pilgrim’s “fears and doubts,” as well as heartache, discouragement, and rejection, pain and despair. disease and death and so on. Our life might be a journey through some strange, distant land like Middle Earth (aka Endórë in elfish) where there are frigid, desert, marshy, rocky, wooded and other landscapes; where little seems familiar, but of one thing we can be certain–we are far, far from home.
Sometimes we must make parts of this journey alone. Fortunately, God has given me a faithful, loving partner who can help shoulder my burdens even as I do hers during this part in our lives.
February 7, 2024 (Wednesday)
Yesterday, I visited my doctor’s office and because things are so blurry right now, I don’t recall the primary reason other than to report dark grey/green urine. I was also concerned about stressing my liver. While there and on a hunch, they gave me a flu test and I tested positive for Type A flu. They also ran a CBC on me (my WBC’s had dropped back to normal which suggests the UTI is clearing up, and my glucose was high at 122, likely because of the flu.). As far as chemistry, my sodium was a bit below normal, but my potassium was still normal. I also received a script for Tamiflu, which usually works for me. For the last forty or fifty years, I’ve gotten my flu shots religiously. Later in the day, Deena was feeling ill with flu-like symptoms. She is on Tamiflu now.
Today, I saw the first proof that I was passing blood per rectum. There was bright red blood on the toilet tissue and in the bowl. We called the urological office to see if the chemotherapy might have caused it, They called back and said “No!” They said I should follow up with my PCP. About 9:30 p.m. tonight, I received a note that my pcp wants me to be evaluated tomorrow.
What could it be? I’m not overly alarmed because I don’t show any signs of bleeding in my lab work and my platelet count is normal, so whatever it might be is either new, or not spilling a lot of blood. The bright red color suggests a problem in the descending colon, sigmoid colon, rectum or anus. The bleeding is painless, so I can put aside and thoughts of external hemorrhoids, but I know I’ve had internal hemorrhoids in the past that can bleed. I’ve also on two occasions had a fistula and they can bleed, but I don’t think it is that.
The other possibilities are inflammatory bowel disease or cancer. I’m a year overdue on my colonoscopy and I’m on a five-year schedule.
February 5, 2024 (Monday)
Another difficult day. I could not start the Amoxicillin until Sunday morning after the pharmacy opened. I felt on the edge of nausea all day, nose running constantly and coughing up sputum. All I ate were three small fruit cups and one piece of toast. No sign of an URI, however. Nothing has changed this past week in my status as a cancer patient. It’s quite possible I have some future sequels of events. My mind was pretty friend and I derailed as far as my blog is concerned from moving forward.
January 17, 2024 (Wednesday)
Next week will be the first anniversary of my bladder cancer diagnosis. It marks the point where a urological oncologist schedules me for surgery in the coming days. At this point next Thursday, it will be the 347th day post-op from my second surgery (and not counting an emergency procedure to correct a complication a day after the second OR date.) I will also have had thirteen chemotherapy treatments by then, three cystoscopies, two CT scans of the bladder, and about thirty-two cheeseburgers.
The cystoscopy I had in June showed a bladder resembling the basement of the Palais Garnier– Opéra where Eric the Phantom lived. There were long mysterious drapes of dark eschar or devitalized (i.e. dead) tissue that swayed like sea grass in the tide. My doctor told me that it was a bit surprising to see so much at that late date, but it was normal. The OR sites from which the cancer was removed appeared normal. as well. At the end of the procedure, she removed a few milliliters of fluid, or bladder washing as it is called, for a cytology specimen. The lab looked at it and concluded “Benign. Reactive urothelial cells.” The best possible news.
Last October I had another cystoscopy. The eschar by then was gone. The bladder looked clean and bright and there was a spiderweb of reddish-colored blood vessels resembling a metropolitan transit map visible through the urothelial lining of the bladder. Cytology showed abnormal, but benign cells.
This is the best approxima-tion I could sketch of what we saw earlier this month.
Last week I had my third cystoscopy. This time there was a noticeable feature not observed before. The bladder walls were once again ivory colored and bright. The blood vessels visible again, but there was an elliptical shape, perhaps an inch or so at it’s widest points. It looked entirely symmetrical and the margins of the artifact were clear and sharply defined. The color of the ellipse was a flat pink, uniform across the entire lesion. It looked mildly inflamed to me. After examining at the whole bladder, the opening of the ureters, trigone and OR sites, my doctor said aloud “Looks like a happy bladder.” Then, a pregnant pause. I could almost hear her thoughts in the thundering silence that followed, and I prompted her by asking about the ellipse. She nodded. She was training a resident who was performing the procedure and she asked him to pass over it again. She didn’t take a photo of it as far as I know and suggested it might be an inflamed area of tissue because she said that the chemotherapy catheter usually lies in that area during chemo treatments and it is possible it was caused by my last (December) treatment. But, she didn’t seem convinced of that to me, nor did she seem unduly alarmed. Instead, she said she’ll make a point of checking the area again in April when I have my next exam. After a second visit to my prostate, the catheter was removed. A few days later, the cytology came back with the following comments:
Urothelial cells arranged in groups, in a voided urine may be an abnormal finding which can be seen in inflammatory conditions, in association with calculi and in urothelial neoplasms. Cytologic evidence of a high-grade urothelial neoplasm is not demonstrated. Clinical correlation is recommended.”
My CT from earlier this month noted “Resolution of previously noted right-sided bladder mass.” That’s good news. Computerized axial tomography is usually very definitive. However, that artifact on my bladder might be two dimensional only, in which case it “might” have escaped detection. Five percent or so of bladder cancers do escape CT detection. My cancer is high-grade, which means there is a good chance of recurrence at some point, but then again, it might not occur. But I won’t be Erwin Schrödinger’s cat this time around.
I feel okay. I’ve made a mental note to examine my urine closely for an sign of bleeding in the day, weeks and months ahead. Other than that, life for Deena and I will go on. We do and plan to thank God for every day we have together. As the poet laureate and Pulitzer Prize winner Robert Frost wrote in his poem Stopping by Woods on a Snowy Evening:
The woods are lovely, dark and deep,
But I have promises to keep,
And miles to go before I sleep,
And miles to go before I sleep.“
I thank God that if I had to have cancer, that it was bladder cancer and not pancreatic cancer, lung or brain cancer, and so on. My chemotherapy treatments are more of a nuisance than a hardship. And I’ve learned that being reminded of your mortality can make you more appreciative of the life you still have. Deena and I do not presume we have tomorrow because tomorrow is not promised to either of us. But we do have today and we have things to look forward to. Thanks for supporting us with your thoughts and prayers.