NOTE: I have two additional aneurysm threads on this blog: How my wife’s aneurysm was first discovered here and additional information on intracranial aneurysms here.
This post is a continuation of a previous post titled Omi’s Aneurysm. In this post, I plan to journal what I hope will be a very uneventful recovery in the days and months ahead following my dear wife’s surgery, which occurred on August 9, 2024 for a 7 mm saccular, intracranial aneurysm. The word “intracranial” means within the cranium, or inside the bones that form the head. More than likely in this context, it refers to the largest of the three structures we know as the brain, and that is the cerebrum.
I want to add additional information in this post that I have not mentioned before. The best place to start is with a narrative summary of Deena’s pre-op health in general.
NARRATIVE SUMMARY
Deena has lived a healthy smoke-free life overall, cancer free, with a healthy heart, liver and kidneys, though her blood pressure would run high because of her family genes. It was only three years ago when Deena was 67 that she consulted a cardiologist who wasted no time getting her blood pressure under control. Yet, even people with normal blood pressure can spike briefly under stress or some other illness, and the same is true for people whose blood pressure is controlled with anti-hypertensive drugs. Deena’s genes also made her vulnerable to aneurysms and stroke (which occurs when an aneurysm ruptures, and in people without aneurysms as well.) For example, Deena’s younger brother had an aneurysm occur which needed surgical intervention. Deena’s mom died at the age of 45 from a stroke (an intracranial bleed.) There is no way to know with certainty today if her mother had a ruptured aneurysm, but there is a good chance she did.
Deena only learned about her aneurysm six weeks ago because she had a sentinel event, in her case, blurry vision, followed several weeks later by an episode of scintillating scotoma (See detailing on what a scintillating scotoma is elsewhere in this post.) Deena’s blood pressure during the sentinel event was enough for us to take her to an emergent care clinic which promptly call and ambulance to take her to a hospital for a CAT Scan. It was the CAT Scan that found the aneurysm. Up until then, she was one of the three to five percent of Americans with a brain aneurysm who don’t know it. Some will not die from a ruptured aneurysm. Many others will.
In my post “Omi’s Aneurysm,” I discussed the risk factors for developing an intracranial aneurysm in the first place. What follows below (reading from the bottom up) is what someone who has had a stent or coil might expect post-op.
MARCH 9, 2025 (SU)
Occipital lobe with cortex- Credit: jamulla (iStock.)
So, Deena had a doppler exam on her carotids to see if her visual disturbances were caused by transient ischemic attacks (TIA’s.) Here’s the reasoning: Visual disturbances like scintillating scotoma (described below) can be caused by several different issues, including changes in the blood flow to the brain, particularly the occipital cortex which lies over the occipital area in the rear of the brain where vision is processed and is highlighted in pink and yellow in the illustration. The term “cortex” translates roughly to “bark” as the bark on a tree. I know from the many occasions of taking my classes to the morgue that the cortex feels like the rough side of a dry scrub sponge. Changes in blood flow can be caused by different things, but because her optical disturbances were only temporary, this suggests that the cause of the disturbances is temporary (transient.)
Now, the main arteries carrying oxygenated blood to the brain are the two carotid arteries in the neck. Just as other arteries on a person’s body can get “clogged up” with cholesterol, other fatty debris and calcium, so can the carotids. When for whatever reason the arteries in a person contract slightly, there may be a slight drop off in the blood flow which would provide less O2 to the brain. The fact that Deena at age 70 has pretty clean arteries elsewhere and particularly in her heart suggested that her carotids were also clean, as the doppler did confirm. So, there was good news on two points. The first point is that her carotids were healthy and the second point is that one possible cause of the scintillating disturbances was ruled out. People who do have an atherosclerotic buildup in the carotid arteries might receive a carotid endarterectomy where the plaque is removed and the artery repaired though angioplasty and stenting.
FEBRUARY 28, 2025 (F)
Scintillating Scotoma. A second look
Adobe stock image modified.
Last evening, and a week after her neurosurgeon gave Deena the “all clear” based on her health, and the most recent MR angiogram, Deena had an episode of scintillating scotoma. The term is based on the Latin word “scintilla” meaning “spark” and the Greek word “skotos” meaning “darkness” and referring to a blind spot that may occur. The spark would refer to the pattern you see and the darkness would be, again, the effect of an overall decline in your visual field. If you ever experience it while driving, you should pull off the road as soon as you safely can and wait for it to resolve. I’ve included a photo of a mouse and what scintillating scotoma “might “look like to you. Obviously, since it is a subjective symptom like “hunger” or “euphoria,” you cannot take a photo of it. But people who suffer from this can recall it easily enough. To some people with this, the jagged lines might quiver or vibrate and other people may see tiny grains of light that “pop.”
Scintillating scotoma (which I’ve spoken about earlier in this thread or the previous one) is an episode of a visual disturbance that lasts about twelve minutes with possible variation from person to person. It is most frequently experienced as an aura, which is a sentinel signal that a migraine headache is about to occur. More on that in a moment.
Deena reported that the lines were in color this time (they are sometimes just black and white) and they were more pronounced towards the middle of her left eye. They also were visible in her right eye but to a lesser extent. In the course of the twelve minutes, the pattern slowly drifted to the left edge of her visual field. She also had photophobia along with the disturbance, and photophobia refers to a sensitivity to light, so when she reported that, I turned the lights in our living room lower to reduce the stress of the experience. We had to wonder whether this was related to her aneurysm, but it was not immediately clear, because she had seen her eye doctor earlier in the day. He ordered some drops and told her to report anything unusual while she was on the medication. The medication was a combination Dexamethasone and an antibiotic. Dexamethasone is a powerful corticosteroid used to treat everything from arthritis to ulcerative colitis to cancer. We called the after hours number and the doctor on call did not think what Deena saw was caused by the eye drops.
There is no direct relationship between Dexamethasone and scintillating scotoma. However, there is the possibility on an indirect relationship. But because she had taken only a single dose of the steroid, it did not seem to fit our circumstance.
We researched to see what medications might cause scintillating scotoma? There were three groups: anticonvulsants, antidepressants, and vasodilators. She is not taking anticonvulsants and antidepressants, but she is taking a vasodilator called Nifedipine. This drug along with nitroglycerine and Verapamil is capable of producing this visual disturbance, namely through the process of dilating the arteries in the brain which lead to changes in the blood flow to the visual cortex, which is the area of the brain that processes, visual information received from the retinas of the eyes. This dilation may trigger visual disturbances such as scintillating scotoma.
Nifedipine also acts on the way your body processes calcium which may contribute to visual disturbances as well. There are also other things that cause scintillating scotoma, but I won’t go into them.
However, if you want to learn more about this phenomenon, your best bet is to check out books on migraine headaches. It was during my migraine headaches spanning thirty-three years that I encountered them, myself. So, clearly most people who know about this also suffer from migraines.
However, Deena does not have a history of migraine headaches. And while she has occasional stress or sinus headaches, she does not have the horrible pain associated with migraines.
So, we consulted our trusty medical AI app marketed to residents and general practitioners and it reported this about silent migraines starting in a 70 year old female:
“Silent migraines in a 70-year-old female can be caused by several factors, including age-related changes in the brain, new onset of migraine with aura without headache, medication side effects, and underlying vascular conditions such as transient ischemic attacks (TIAs). Additionally, hormonal changes and comorbidities like hypertension or diabetes may contribute to the development of silent migraines in this age group.
Silent migraines, or migraines with aura without headache, in a 70-year-old female require careful evaluation due to the atypical presentation and potential for underlying conditions.”
This morning, we started a conversation about seeing a neurologist. We’re not concerned about some other aneurysm or a tumor affecting her brain because it would have been picked up by the CT-scans from last year. However, she might have the early stages of a blood flow issue which is exactly what a transient ischemic attack is, so we will likely follow upon it as a precaution, even though she does now have any other of blood flow or “mini stroke” signs or symptoms. It is possible that her carotid arteries might need to be examined.
In fact, she saw her cardiologist just as I finished this entry and he ordered an ultrasound on her carotid arteries for next Tuesday. Sometimes, plaque builds up in the carotid arteries in the neck just as it does in the arteries of the heart. This has the potential to temporarily slow down the blood supply to the brain if the arteries in the body constrict.
FEBRUARY 21, 2025 (F)
My wife saw her neurosurgeon for hopefully the last time until 2026 yesterday. He took her off her anticoagulant (but she remains on 82 mg of aspirin each day for the rest of her life.) No restrictions on her activity. Everything looks good.
Deena had what might have been a close call, and she elected surgery rather than wait and hope for the best. The surgery went off without a glitch and all she has today are occasional headaches which may easily be sinus or stress related since her aneurysm does not exist any longer in any functional way.
I will continue posting news and tips on intracranial aneurysms, however, as this has turned out to be one of my more popular threads on my blog. If you would like to contact me please use the comment section of this post and I will answer you promptly.
May God bless each and every one who comes across this note. I wish you health and all the best.
– More to follow –
FEBRUARY 14, 2025 (F)
Today, Deena had her six month post surgical MRA (magnetic resonance angiography) which checks her blood vessels for blockages, clots and aneurysms. There was no contrast involved. Her twenty minute test was at 11:00 a.m., and we had a copy of the report on the portal about four hours later. We won’t get official word on it until the middle of next week when she sees her neurosurgeon, but we think it looks good. Here is the impression of the radiologist after he compared today’s results with the MRA from last July:
“Flow diverting stent extending from the clinoid to the communicating segment of the right internal carotid artery. Previously identified aneurysm at the right carotid terminus does not demonstrate flow related signal, appearing excluded.”
We discussed it quietly for a few moments. What was the radiologist saying? It was like we were trying to read tea leaves or something, but I couldn’t see any red flag in those thirty-three words. Finally, I typed the impression above into a medical AI program I have on my phone. This program is designed for residents and internal medicine practitioners, and I asked it for a paraphrase of the impression above. My phone clicked and chirped a few seconds like a cricket before the program responded and said that the lack of a signal suggests that there is no blood flowing through the area where the aneurysm was previously noted, because what was previously seen as the sac of the aneurysm is either withered away, or permanently sealed off or firmly clotted with blood. The program also said that if surgery was performed on the aneurysm, then the surgery was likely successful. What remains is a confirmation from the surgeon next week that the stent has not moved since he placed it (he will have the images on his computer) and we’re hoping she can come off blood thinners with the exception of aspirin (82 mg/day for the rest of her life.) But we feel good about the decision to have it surgically treated. She still has occasional headaches which can be explained by ordinary, everyday stress and she has not had any visual effects (scotoma) since Thanksgiving. A year from now, she may get a follow-up MRA. All that is left is to thank God for revealing this potentially life-threatening aneurysm before it ruptured and for guiding the hands of the neurosurgeon during the procedure.
I peruse comments everyday on intracranial aneurysms and I am painfully aware that for every success story there are tragedies to match. For those people stricken with stokes from a ruptured aneurysm, our hearts ache and we are left deeply humbled. Please contact us using the comment section to this post if we can be of any service or encouragement to you or your loved ones who are traveling on the same path we did. We wish you well.
DECEMBER 24, 2024 (T)
Wow! It’s almost the end of the year already. I have two reasons for adding this postscript. The first is provide everyone of the eight hundred or so people who have visited this post some information on how Deena is doing almost five months post-op, and secondly, to provide a potentially important caveat for those readers or their friends and family who might have an intracranial aneurysm.
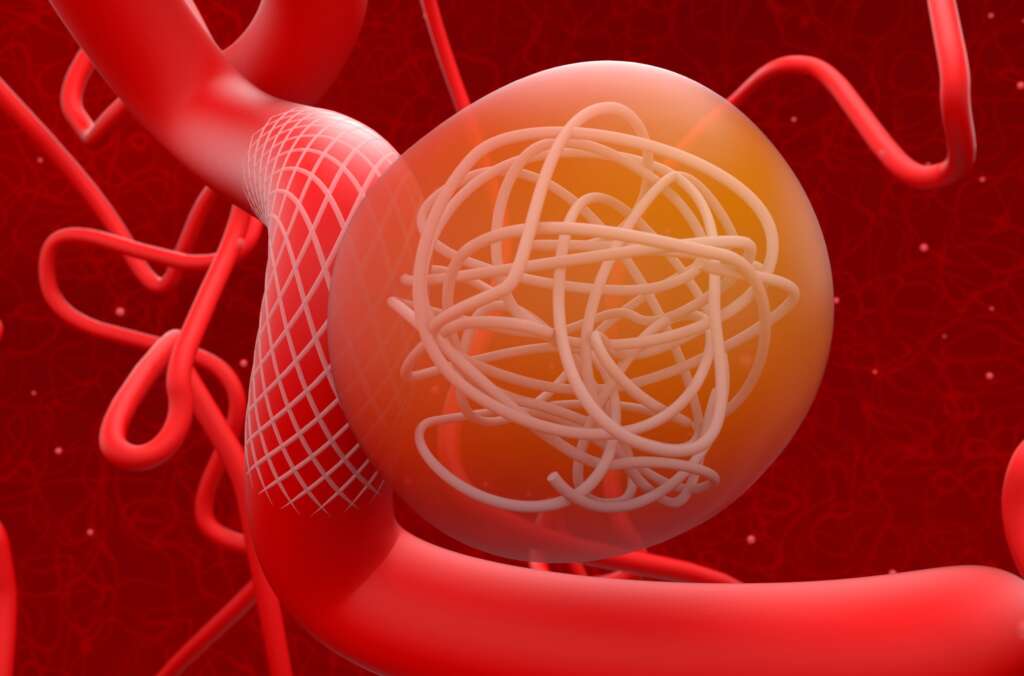
Coiled and stented intracranial aneurysm. Not every cerebral aneurysm may be treated this way. Illustration credit: Nemes Laszio (Dreamtime.)
Deena saw her neuro-surgeon around the middle of November. He was very pleased, though she is not quite done with him yet. She has a cerebral angiogram (to be scheduled) sometime during the next sixty days to be sure the stent is still in place and that the aneurysm is still sealed off. Then, she sees him again afterwards this spring to discuss the findings. Beyond that, she may require annual CT-scans, especially since she has another smaller aneurysm in one of her sinuses (I think it is in the cavernous sinus at the base of her brain not too far from the original sinus.) These sinuses are not to be confused with the sinuses people have around their nose.
So, after almost five months, Deena’s blood pressure is almost always normal, thanks to Valsartan (an anti-hypertensive medication) and Nifedipine (a potassium blocker), often given to heart patients, though Deena’s heart is in excellent condition. A year ago, she was getting four or five headaches a week, but now maybe only one headache every week. She gets a minor nose bleed once every month or so at night from the blood thinner. She had a dental cleaning earlier this month and because her teeth and gums are in excellent condition, that was not a problem,either given the blood thinner. We both feel blessed by God at this happy outcome.
For the second issue, I happened to read a post on social media from someone whose husband had a ruptured aneurysm and the poster wondered whether obstructive sleep apnea might have caused the rupture. Once again, I am not a doctor, so if what I am about to write interests you, then by all means seek competent medical advice and take no action solely on what I write. I checked into this issue this using a medical decisionmaking AI tool, and it reported that there is a relationship between CPAP use (not obstructive sleep apnea itself) and ruptured aneurysms. Here is what I found (Pathway CME 0.5):
“CPAP can increase intracranial pressure due to the positive airway pressure it provides. This may pose a risk for patients with intracranial aneurysms, as elevated intracranial pressure could potentially lead to aneurysm growth or rupture. CPAP can cause hemodynamic changes, such as decreasing right ventricular output and impeding systemic and pulmonary venous return, which may affect intracranial pressure.
The relationship between CPAP use and intracranial aneurysms is not well-established. However, the potential increase in intracranial pressure from CPAP use may pose a risk for patients with existing or potential aneurysms. The limited and mixed evidence highlights the need for individualized assessment when considering CPAP use in patients with intracranial aneurysms. Clinicians should weigh the benefits of CPAP, such as improved oxygenation and reduced apnea-related spikes in blood pressure, against the potential risks of increased intracranial pressure in patients with intracranial aneurysms. The decision to use CPAP should be individualized, taking into account the patient’s specific condition and needs.
In conclusion, the relationship between CPAP use and intracranial aneurysms is complex and requires careful consideration of the potential benefits and risks. Individualized assessment is essential, and further research is needed to better understand this relationship.”
Nor should someone who has been on CPAP therapy for some time suddenly stop using it without consulting their physician, because suddenly denying your body an advantage it has enjoyed over time can cause other (heart-related) issues as a consequence.
Usually, there is only a certain amount of information that a clinician (doctor) provides a patient and he or she does not include every possible scenario, else the patient would be overwhelmed with information, much of it not applicable to their circumstances. But when I read this, it seemed important enough to add to this blog, given the sheer number of people using CPAP today. So, for what it’s worth . . . and please run it by your doctor if (1) you have an aneurysm and (2) you are using a CPAP. Take no arbitrary action on your own.
Deena and I wish everyone who reads this a Happy Holiday and God’s blessings on you and yours.
OCTOBER 9, 2024 (W)
It’s been two months post-op after the flow diverting stent was inserted in Deena’s aneurysm. No unusual optical effects for the past two weeks, blood pressure is really good x 10 days thanka to the Nifedipine, and headaches seem to be resolving a bit. The only unusual S/Sx are occasional nocturnal nosebleeds (one last night and the other a week or ten days ago.) They are easily controlled and welcome–at least to me–because it is the blood thinner telling us that it is still working while epitheliation continues.
SEPTEMBER 22, 2024 (SU)
Bad headache yesterday in the back of Deena’s head for much of the night before and most of the day. Did not resond very well to Tylenol until late. Blood pressure has been normal the past two days, however. I am fairly sure that Deena’s optical disturbances (i.e., scintillating scotoma) are probably caused by a small amount of inflammation or perhaps small, almost imperceptible changes in the flow of blood around the location of the stent. This is likely unavoidable. But if true, then the frequency and the degree of disturbances are possibly related to the degree of inflammation. I expect over time that this will resolve.
Again, there is not very much published, professional research in this area, and the authors of those articles that are available admit that there are many unanswered questions. Our plan is (1) to see a retina specialist as soon as possible to see if there are any subtle differences that he can note, and (2) monitor what Deena is experiencing and keep her neuro-surgeon in the loop as far as changes or other emerging issues go.
IMPORTANT NOTE: For anyone who reads this (and I have a hundred or so people every week who visit this post from a dozen countries around the world), please do not accept what I write as professional advice or try to apply it to your experiences. Everyone is different, with different states of health, on different medications and so on. My comments are purely empirical and possibly subject to error. You should follow your doctor’s advice without fail or deviation.
SEPTEMBER 18, 2024 (W)
The Nifedipine Deena’s cardiologist prescribed seems to be improving her blood pressure. The systolic occasionally rises to the 150 range, but is increasingly normal. So, that’s a relief.
HIGH BLOOD PRESSURE
Under pressure.A once sturdy pier in a state of collapse from the effects of the pounding surf. Photo credit: Martin Tosh (iStock.)
Deena has had lifelong hypertension, which is a major factor in the development of brain aneurysms. And except for some “skipped beats” a few years ago, her heart seemed to be sound. So, why does she have a cardiologist? It is literally a long story. Year-after-year earlier in her life, whenever she saw a doctor, she was told that her blood pressure was high. Maybe 140/90 or something like that. But for decades, no one worked her up or treated it specifically. When she went to the ER while on a trip to Texas three years ago, I talked her on her return to New York into seeing a cardiologist, because I knew a cardiologist would be more likely to diagnose and intervene than a family practitioner (no slight intended towards family practitioners who do excellent work. Sometimes, you just need a specialist.) If I had my choice of a cardiologist, and depending on what my problem might be, I might choose an interventional cardiologist rather than a general cardiologist. The reason is, interventional cardiologists are trained to do invasive procedures, such as heart catherizations, cardiac ablations, etc. So, they might make different choices for you well before you need these treatments with the understanding that they might have to invest in your care to a degree that a general cardiologist would not. And like family practitioners, I have a great respect for (and have worked with) general cardiologists. My point in this paragraph is to advise you to get your high blood pressure under control before it ruins your kidneys and eyesight and particularly before you develop intracranial aneurysms. The arteries, arterioles and capillaries in your brain and other vital organs cannot stand the incessant pounding caused by hypertension. They are like a structure on a sandy beach where frequent hurricanes, tropical storms and high tides just weaken the structure over time until they fail and fall.
SEPTEMBER 15, 2024 (SU)
A BRIEF HISTORY OF FLOW DIVERTING STENTS
I wanted to add a bit more about flow diverting stents (FDS) that are used more and more to treat intracranial aneurysms. These are relatively new devices (the first flow diverting stent was approved by the FDA for use in 2011.) So, clipping and coiling have historically been the more common approaches to repair aneurysms. Clipping requires that the surgeon makes a small opening in the patient’s skull. There are risks as in any surgical procedure. With clipping, the risks include stroke like symptoms, infection, headaches and so on. But clipping often produces better outcomes. Coiling, on the other hand, is less invasive and safer, especially if the patient is older or has other major health risks. Perhaps, it is because coiling is less stressful to the patient than clipping. As an article from Cureus on the National Institute of Health site notes:
“Neurosurgical clipping provides better results in terms of mortality, re-bleeding, and re-treatments. Endovascular coiling is a better surgical technique in terms of post-operative complications, favorable outcomes, and rehabilitation.”
With coiling, a flexible tube is inserted typically in the patient’s wrist or groin and threaded through the various arteries until the aneurysm is reached. Fluoroscopy allows a live-time visualization of the aneurysm as the platinum coil is inserted (See short video here.)
Early attempts at coiling, were not completely satisfying, so stents were developed to cover the entrance to the aneurysm to keep the coil in place and to ward against debris such as micro clot fragments from entering the bloodstream. It wasn’t long before the stents became a treatment all of their own, especially if the entrance to the aneurysm was particularly wide.
SEPTEMBER 14, 2024 (SA)
People who have had aneurysms repaired, at least with stents, often complain of headaches. Just now, my wife Deena who is five weeks post-op from having a flow diverting stent threaded to the entrance of her aneurysm, had another scintillating scotoma episode, this time in her left eye, lasting the typical fifteen-to-twenty minutes before disappearing to the left (outer) edge of her visual field. I checked her pupils and they were equal and responsive to light. This visual disturbance, which was confined to her left eye and described elsewhere in my blog, was an aura or precursor to a headache that emerged twenty minutes later on the right area of her head, behind her right eye. While experiencing the scotoma, she also reported a decrease in the peripheral vision of her left eye. This is all anecdotal, of course, because we have no way of measuring or verifying any of this clinically. Nor do we have the knowledge and judgment of a physician to guide us. But this may resonate with those people who have had stents implanted and help them understand that at least they are not alone concerning their experiences. We hope to have an in-depth examination of her eyes, particularly the retina, in the near future.
POST-PIPELINE HEADACHES
People who have received flow diverting stents complain routinely on the intracranial aneurysm discussion boards of headaches. In fact, after researching this phenomenon, I discovered something which is called a “Post-Pipeline Headaches” This journal article from 2020 begins by noting:
Flow diversion using devices such as the “pipeline” stent is now a common treatment for unruptured intracranial aneurysms. Though much is known about the efficacy of the device, less is reported regarding potential side effects. In this study, we report the frequency and characteristics of the “post-pipeline headache.”
HEADACHES
Most people have had different types of headaches at different times in their lives. Probably the first headache that comes to mind is the migraine headache. Onset often occurs in adolescence and continues throughout the early life of the patient, with many patients having experienced their last migraine in their mid-forties, as was the case with me. My migraines caused me to miss several days of work each month, and they usually resolved after episodes of nausea and violent vomiting, which typically lasted twenty-four hours or so per episode. Nothing I tried could stem the pain in the meanwhile. Invariably, I would go to the local emergency room where they knew me well. I would get a shot of 50 mg of Demerol for pain and 25 mg of Vistaril for nausea and vomiting. Then, they would pat me on the behind, and send me home to sleep it off.
The article cited above defines Post-Pipeline Headaches as “a new headache or pain distinct from their prior headache syndrome.” This is true in my wife’s case.
The conclusion is:
Post-pipeline headache is common and can occur in up to 50% of individuals undergoing the procedure. It is more common in younger individuals with prior headache history, and has distinctive features. While symptoms can remit over time, up to two-thirds endorse ongoing headaches. Associated features such as co-existing visual, cognitive, motor, or vestibular disturbances make ongoing headache more likely and suggest that the lingering headache syndrome may fall along the migraine spectrum.”
From this study, we can infer that one out of two people who receive stents for the purpose of resolving their intracranial aneurysm will experience headaches, especially if they have a history of chronic headaches or migraines prior to the surgery. We also see that this Post-Pipeline Headache is more common in younger patients, and while it often feels different than other headaches they have experienced in life, it is not dissimilar to migraine headaches with “co-existing visual, cognitive, motor, or vestibular disturbances.” In the case of Deena, the disturbances are visual (scintillating scotoma.). It can also be, and as is the case with Deena, photophobia, or sensitivity to light.
WHAT MIGHT YOU EXPECT?
Cognitive disturbances might include problems with “processing speed, attention, memory, verbal skills and executive functions.” Motor disturbances—when they occur—are often impairment in speech, numbness or weakness.
Vestibular differences might include vertigo, problems with balance, nausea and vomiting.
COULD INFLAMMATION BE THE CULPRIT?
An abstract from last year in the AHA Journal suggests that the placement of a stent can cause an inflammatory response in the tissues adjacent to the stent. Citing an actual patient, they note:
We found MR imaging evidence of perianeurysmal brain inflammation after the therapeutic thrombosis of the sac to be the main cause explaining clinical aggravation.”
The patient’s physicians tried a procedure called Pulse Steroid Therapy on the patient. After a course of this treatment, the researchers noted:
We experienced a significant improvement in the patient’s clinical findings and contrast‐enhanced MRI findings after steroid treatment.”
So, this is a possibile treatment that is emerging. Again, a lot is unknown for patients who develop headaches after aneurysm repair with a flow-diverting stent.
Often, but not always, these S/Sx described above resolve by themselves over time, but many other patients continue with some degree of pain or discomfort.
I hope this has been helpful for those patients recovering from an intracranial aneurysm aneurysm repair.
SEPTEMBER 13, 2024 (F)
Deena continues to have high blood pressure readings and headaches. Her blood pressure is generally 165/100 or so. Her headaches are just behind the right eye or along the side of her head. Her cardiologist returned from vacation and put her on Nifedipine, a calcium blocker with the expectation that it will lower her blood pressure. She had her potassium tested this week and it came back just above the lower limit of normal, so we are thankful for that.
This afternoon, however, as Deena felt faint and felt as if the room were spinning around her, I checked and she had a blood pressure of 88/42, no doubt from the Nifedipine. Her doctor told her to break the table in half and just take 1/2 tablet each day. This seems to be working.
She is now into her second post-op month which is a relief as most complications from an aneurysm take place within thirty days of placement.
SEPTEMBER 5, 2024 (R)
This is probably a good place for me to remind readers that I am not a physician, not can I legally provide medical advice. My blog simply provides what I hope is reliable survey of the literature on different topics in international affairs, science, religion, history and health. In matters of health, you should always follow the advice of your health care providers.
Deena continues to have borderline hypertension ~140 to ~160 systolic pressure and a diastolic pressure (thankfully) less than 100. This may be because her cardiologist’s office has been adjusting her blood pressure medicine and her potassium intake as she moves through her first month post-op. Or, it can be ordinary stress. However, we have some angst about the effects of the mildly increased pressure on her post-op site where the stent shuts off the former aneurysm. We don’t know for sure if this can be a problem, but certainly very few people benefit from high blood pressure, aneurysm or not. Because potassium plays an important role in the function of the smooth muscles in the arteries, the absence of adequate levels of potassium tend to temporarily reduce the elasticity or suppleness of the arterial walls somewhat, thus increasing the pressure. Deena and I talked about setting a “red line” of 185 systolic and/or 115 diastolic, at which point we’d make an unscheduled visit to a clinic. Last night, her blood pressure was up slightly when we retired for the evening. This morning, it is normal, thanks be to God. Obsessing over it can also raise the value.
I wanted to include some more important or interesting facts about aneurysms for the many people who follow Deena’s progress. Today, I’d like to talk about a tool that neurosurgeons use to evaluate a person for surgery. This tool is called a PHASES score. I’ve included a link to the template so you can calculate your own risk if you know you have a brain aneurysm.
PHASES stand for “Population,” “Hypertension,” “Age,” “Size of the aneurysm” “Earlier hemorrhage from an intracranial aneurysm” and “Site of the current aneurysm.” In terms of population, physicians know that people of Japanese or Finnish ancestry pose additional risks for rupture. High blood pressure, which is abbreviated as “HTN” in your medical records, increases the risk since any sort of pressure would cause stress something. This is why there are weight restrictions for elevators, maximum pressures for when you add air to the tires of your car, and so on.
And incidentally, the medical transcription term for low blood pressure is “htn.”
All other things being equal, it seems logical that the larger the aneurysm, the greater the chance for either rupture, or at least the aneurysm causing other issues in your brain because of its sheer size. The site of the aneurysm is an important factor. Why? Because when a brain aneurysm ruptures, there are only two places for the blood to go. It can seep into the brain tissue, itself (what is made of grey and white matter and called the parenchyma), or it can leak into the tissue surrounding the brain, in this case, the subarachnoid space. Here, it increases the pressure on the brain, which cannot harmlessly expand as the tissue in your wrist or ankle does when it is injured. There is just no room in the skull for more fluid. According to the National Institutes of Health
“When an intracranial aneurysm ruptures, it may bleed into the brain parenchyma resulting in a parenchymal hemorrhage, or more often, it will bleed into the subarachnoid space, resulting in a subarachnoid hemorrhage (SAH). A SAH is a catastrophic event with a mortality rate of 25% to 50%.”
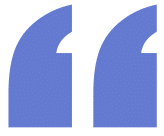
Close-up of the meninges. CSF and Membranes that envelop the brain. Credit edesignua (Deposit Photos.)
There are three basic linings around your brain and spinal cord. These layers are called the meninges and they function to protect your central nervous system. The outermost is the dura mater, the innermost is the pia mater, and in between the two is a layer called the arachnoid (names for spiders because of its spider-like appearance to it.) The subarachnoid space is the space between the arachnoid and the pia mater. It is in this subarachnoid space that your cerebral spinal fluid (CSF) is found. The CSF serves as a cushion or shock absorber for your brain to protect it from injury. This is probably why God placed our heads at the top of our bodies—to protect our brains from injury. Now, that comment might seem funny or weird, but there are researchers called “astrobiologists,” science fiction writers and Hollywood directors who consider points like this when they speculate on what extraterrestrial life forms might look like. A Martian might have green skin and bloodshot eyes, but it would be at a disadvantage if its head was just a foot off of the ground.
Now, let’s look at why certain populations contain higher risks. What is different between Japanese and other Asian people such as Chinese or Koreans and between Finns and Danes or Russians? Or, are there genetic similarities between People from Japan and people from Finland?
-More to follow shortly-
AUGUST 30, 2024 (F)
It’s been exactly three weeks since Deena had her stent put in to resolve her brain aneurysm. For the past week or so she gets “winded” easily, and her famiy and friends notice the shortness of breath, sometimes even when speaking while at rest. It is barely perceivable, but noticeable. Because her sinuses have been acting up, probably allergy related, we wondered whether it might be a sinus infection brewing with some conjestion beginning in her lungs. She had a productive cough (as opposed to a dry cough) and was bringing up sputum. She also mentioned some tinges of blood on her Kleenix. Now, old age has robbed me of my common sense in some cases, so when I hear “hemoptysis,” I think of tuberculosis, pulmonary edema, and so on (i.e., zebras, not horses.) The fact that Dee is on blood thinners did not register to me at the moment, and that was a perfectly logical explanation. In fact, the preferred answer.
We saw a PA on Wednesday and a doctor on Friday (outpatient appointments.) I was hoping they would run a CBC (complete blood count) because I suspected that maybe Dee had a low Hemoglobin count which would explain the shortness of breath. Normally, the molecules of oxygen in the lungs bind with the atoms of hemoglobin and this is how oxygen is transported through the bloodstream to the organs in the body (including the lungs, themselves.) The lower the iron (hemoglobin) count in your blood, the less oxygen is reaching the cells of your body. You are now anemic. In fact, it was probably a good thing the PA and doctor did not run any blood tests, because other values on the CBC would likely have been low as well, raising further concerns. The reasonable conclusion to Deena’s presentation is that this is all a result of the blood thinner she is on, and an out-of-whack blood chemistry probably explains why she doesn’t feel quite right. What the doctor did do beyond a careful physical exam (especially listening for breath and heart sounds) is to perform a swab test for COVID and flu which came back negative, and order a chest x-ray. The x-ray showed that Dee’s lungs were within normal limits with no sign of congestion, and that reassurance is helping us through Labor Day weekend.
So, it just takes time.
AUGUST 26, 2024 (M)
Deena had a good week. Very few headaches, and those few she had were not severe. No visual disturbances. Blood pressure ok, though her systolic pressure occasionally creeps into the ~150 range. She is back to her normal routine. It took her almost two weeks to engage herself socially again (she sort of eased into it), but except for feeling tired during the day and some problem sleeping at night (which is not unusual), we’re putting the aneurysm repair in our rear view mirror. Technically, her first month pre-op which is the most risky period after an aneurysm repair has another two weeks to go, but as of now she seems fine. She’s still on Prasugrel (a blood thinner) and will remain on it until at least the end of the year. After that, there will be another IR-Angiogram. Next month, she is planning on a visit to Florida and late next Spring, a trip back to Ireland. She, her sister and a mutual friend will spend some time in Belfast and the counties around County Antrim. After that, they will spend a few days with the Puffins rehabilitating/restoring the birds’ natural habitat (or something like that.)
Puffin in Ireland waiting to meet new friends from New York State. Photo credit: Patryk (Adobe.)
Deena wrote a very nice note to her surgeon explaining who she was, some of the many activities she is involved in and why the repair was important to her. Surgeons rarely have much personal interaction with their patients compared to other medical practitioners, so this gives her surgeon the opportunity to know her better and the celebrate the happy outcome. We’ll leave the rest of the recovery in the hands of our loving Heavenly Father.
p.s. For those who have a Facebook account, if you search for “brain aneurysms,” you’ll find several Facebook sites with many thousands of survivor accounts, including those patients, both pre- and post-op, and how they are coping. I highly recommend it. Meanwhile, please visit this site every week or so for additional useful information on Deena an/or intracranial aneurysms. Also, the Brain Aneurysm Foundation has many useful videos which helped us understand the risks and benefits and adjust to her surgery.
AUGUST 21, 2024 (W)
Deena had her surgical follow-up this morning. She was cleared for normal activities (e.g., driving, working around the house, social activities, flying and so on.) She has another follow-up with the surgeon in three months and she continues with her anticoagulant meds. We wanted to know if in the future she needed any blood tests to check her clotting factor but were told they were not needed because the drug she is on is generally reliable. We also asked a bit more about where the stent is located vis-à-vis other organs and nerves and it seems it is closely located near the Ophthalmic nerve. The nerve, itself, which is only one inch long, is intricately woven into two other cranial nerves (the Trigeminal and the Optic nerves.) Damage (or simple inflammation) to the Ophthalmic nerve is expressed as:
Relatively sudden decrease in vision, such as blurring, darkening, or dimming of vision; Loss of vision in the center of, part of, or all of the visual field; Abnormal color vision, such as dull and faded colors; Pain in or around the eye, which is often made worse with eye movement.”
I asked Deena’s neurosurgeon if the presence of the stent just upstream from the Ophthalmic nerve, through an almost imperceptible change in blood flow dynamics might account for the several episodes of scintillating scotoma Deena has had, and while he couldn’t know for sure, he did not appear to be concerned. This optic phenomenon might just be from the insult to the small area of the brain as the stent was placed. In that case, it should resolve without further sequelae. Fortunately, there does not appear to be any reason for alarm. Fortunately, and in contrast to the reported experiences of a few other post-op intracranial stent patients, Deena has not had unmanageable or painful headaches. Those headaches that she has respond to Tylenol.
So, that was just a theory.
AUGUST 18, 2024 (SU)
Nineth day post op. Deen felt relatively well yesterday, did a good deal of work around the house (but no heavy lifting.) This morning, she has a bad headache on one side of her head with pain in her left leg. Her blood pressure (specifically her systolic pressure which measures her heart as it works, was up.) This may be due to the pain she is feeling, as pain tends to raise blood pressure. She took her morning meds, some TylenolTM and an Oxycodone and will try to sleep it off (this was the second consecutive night where she did not get much rest.)
Nurses and many doctors practice what is called “SOAP” charting, and it is a good way to train or regiment yourself if you are a caregiver. The “S” stands for “subjective,” usually what the patient reports she is feeling, whether faintness or fear, pain, and so on. The “O” stands for “objective.” What can you as the caregiver record or observe, such as a fever (or not), the pulse rate, a rash, disorientation, etc.? “A” stands for “assessment.” What do you perceive as the patient’s present condition? Are they having trouble speaking, standing, staying awake, and so on? FInally, “P” stands for “plan.” What do you intend to do about the situation? In this case today, I plan to check on Deena regularly (but not constantly) as I think she will do better with sleep and pain with the analgesics. If I check every fifteen minutes, she won’t get and rest.
Without knowing how things will be by lunch time or this evening, today so far is a reminder that recovery from this surgery (any surgery, or any illness) is a bumpy road.
For patients who have had an aneurysm repair, especially if it involved the insertion of a stent, the first month is the time period when a patient is more susceptible to a clot forming or some other post operative complication developing. But aside from any serious problems arising, each day means your body is adjusting more and more to your stent, and time is likely on your side.
AUGUST 16, 2024 (F)
It’s been exactly a week since Deena had her surgery (See below and here.) All in all, the first post-op week went well. Yesterday there was another (second) episode of a visual disturbance which lasted just under twenty minutes. It is an event, in that there is a clear time when it starts and a time it disappears. It seems to match the description of scintillating scotoma (described below.). But there have been no frank stroke-like symptoms or anything to suggest something is amiss. Deena did not sleep well last night, but that is not unusual in itself. She has had some headaches the past week, but TylenolTM usually eases the pain. She feels worn down and weaker than normal (struggled lifting a milk carton recently), though she has walked around the block. These limitations were anticipated. Her brain is just recovering from the insult of the procedure.
We pay close attention to her taking her meds as scheduled. She takes her blook thinners when she wakes up. We understand there is a certain amount of stroke risk during the first month following surgery as the stent is a foreign body as far as her brain is concerned. At the moment and until the inside of the stent develops a thin layer of living tissue, there are all sorts of nooks and crannies in the surface of the stent for a embolus to develop. Perhaps some patients forget to take their meds, or perhaps the meds are not producing the desired anticoagulant effects in terms of platelet counts, clotting times or however they work? I read a report recently that I cannot locate at the moment that said for post-stent placement patients who have had an intracranial aneurysm repair, the most common time of the day for a clot to form (i.e. S/Sx of a stroke to appear) is in the morning., so we don’t want to be late taking a dose for her blood thinners.
TRIGGERS THAT CAN CAUSE AN ANEURYSM TO RUPTURE
The following everyday activities can cause an unstable aneurysm to rupture:
Sudden outburst of anger, getting startled or another strong emotion.
Intense (vigorous) physical activity including lifting heavy objects, moving furniture, etc.
Straining while having a bowel movement.
Blowing one’s nose forcefully.
Recreational drugs.
Sexual activity.
Coffee consumption.
Cola consumption.
Of these triggers listed above, coffee consumption and intense physical activity were the most common triggers in an article in Stroke magazine. There are Online scales that physicians can use to approximate the five year risk of an existing aneurysm rupturing. Using this scale, I estimated Deena’s odds at 1.3%. However, the scaling system (called PHASES Score) is based on a limited number of cases from essentially two racial groups. It does not take into consideration gender and other factors. One concern Deena and I shared as we weighed the options was that if we waited for the time being and intervention was required five or ten years from now, the repair of the aneurysm, itself, or other health issues that might develop might make the procedure very difficult and risky if possible, at all. Deena travels frequently abroad, and the possibility of a stroke while visiting another country would be just too chaotic to contemplate.
Scintillating Scotoma. Today (four days post-op) Deena experienced a fifteen minute episode of scintillating scotoma. She had her first episode about two weeks go following a MRA (Magnetic Resonance Angiogram.)
The etymology of the word scintillate“has its roots in the Latin wordsscintillare, meaning ‘to sparkle,’ and scintilla, meaning ‘a spark.’The verb scintillate is related to the adjective scintillating and the noun scintilla.” The word scotoma referes to a “darkening” defect in a person’s visual field.
Most people see “geometric shapes, shimmering arcs, kaleidoscope colors, and zigzag patterns” and typically as an aura to migraine headaches. The pain of the headache follows the scotoma, though later in life, the scintillating scotoma may continue to appear, but without any pain.
“This atypical brain activity is what causes the so-called visual show and has been linked to a number of health conditions beyond migraine with aura and visual migraine without headache. These include seizure, stroke, multiple sclerosis, glaucoma, stress, head injury, food allergies, hypertension, pregnancy, and preeclampsia. The creation of these electrical impulses has also been linked to high blood pressure, inflammation, and hormonal changes.”
The phenomenon behaves something like static on a television screen before smart TV’s and streaming cable content were marketed. You would have your video on the screen, but would also see the pesky interference from static Yet, scintillating scotoma is not confined to just people with migraines.
STENTING FOR INTRACRANIAL ANEURYSMS
For the present I do not want to discuss the alternative approaches to aneurysm repair, including clipping and coiling. Suffice it to say that Deena’s neurosurgeon believed that a stent was not only preferable over the other options, but that there was really no choice based on how the aneurysm presented itself.
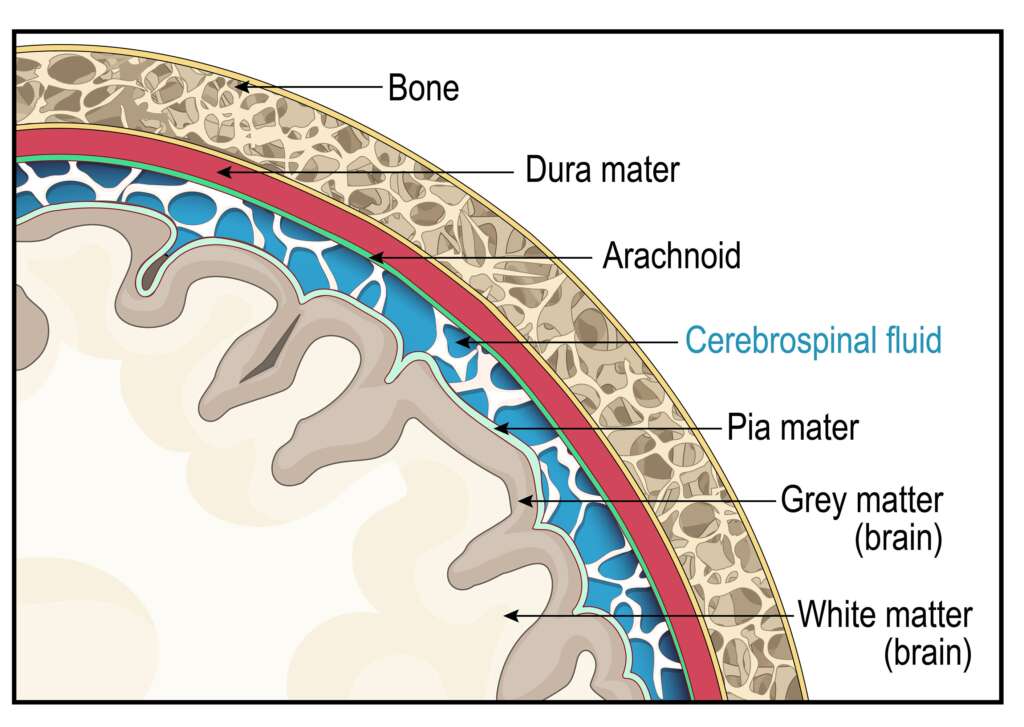
This is what Deena’s stent looks like.
Stenting has only been approved by the FDA for use in intracranial aneurysm treatment since 2002. So, in this context it is a fairly new approach. Deena’s stent is called a flow diverting stent. It makes slight modifications in the flow of blood through the major artery. Flow diversion stenting is a more recent approach (2007.)
Johns Hopkins mentions a number of advantages to a flow diversion stent for intracranial aneurysms, including:
Increased safety: This treatment method eliminates the need for doctors to enter the aneurysm itself — which is often the riskiest part of an endovascular approach.
Shorter recovery: Many patients who once needed extensive surgery can now undergo this procedure and go home the next day. Some patients return to work within a week.
Less recurrence: This technique appears to reduce the recurrence rate (the chance a patient will develop another aneurysm).
Less radiation exposure: In this procedure, patients receive a much lower radiation dose than with other endovascular techniques.
Lower costs: This surgery costs less than other endovascular treatment approaches.
However, there are disadvantages as well to this approach as well.
How many times have you seen a television commercial for medication designed reduce wrinkles or clear up a rash? There are all sorts of warnings you need to be aware of if you use it and a television commercial might scare you to death: “May cause liver failure.” “Patients may develop tuberculosis.” “Have suicidal tendencies . . .” “Linked to colon cancer . . .” People taking this drug should not be pregnant or even plan on having a baby. . .” Ever. You’ll be stuck with cats for company for the rest of your life. And you may have trouble convincing people to vote for you if you ever do run for president.
There are pros and cons that lead you to get your aneurysm treated, and there are sometimes, but not always, choices on how it can be done. This is also true for flow diversion stents:
In English, this means that blood clots can form, creating stroke-like symptoms, possibly with grave outcomes. Your blood thinners that you must take to avoid clots may cause bleeding elsewhere in your body. Over time, the passage way for blood in your stent might narrow for some reason make another procedure necessary and the slight shift in your bloodstream cause problems for the increasingly smaller arteries downstream from the stent.
August 15, 2024 (TH)
Deena continues to slowly improve day-by-day. Her activities are limited by her discharge instructions. No lifting more than five or fifteen pounds, no driving, and so on for two weeks or a month (there seems to be a bit of confusion here, at least in my mind.) She has mild headaches on most days, but they are not the sort of overpowering headaches that some patients report after having their aneurysm repaired. She does have some very mild issues with attention and processing what she reads, but we understand that this is common to most who have gone an aneurysm repair. Deena moves about the house, talks to family and friends on the phone, does light housework and is generally busy with something all day. We are thankful for Facebook sites such as Brain Aneurysm Survivors with fourteen thousand members and Brain Aneurysm Warriors. These online communities allow us to learn from the experiences of others, while sharing Deena’s own discoveries and perspectives. We watch a movie or two together almost daily now. At the moment, she appreciates those simple things that others may overlook or not have time for. We wondered yesterday whether this period might not be a time of personal growth, and she told me about Julia Louis-Dreyfus, whose podcasts were recently recommended to her. Deena has limited stamina, so she is no hurry to be “out and about.” I expect her to return to her normal self in the weeks ahead, but one can never know what God has instore.
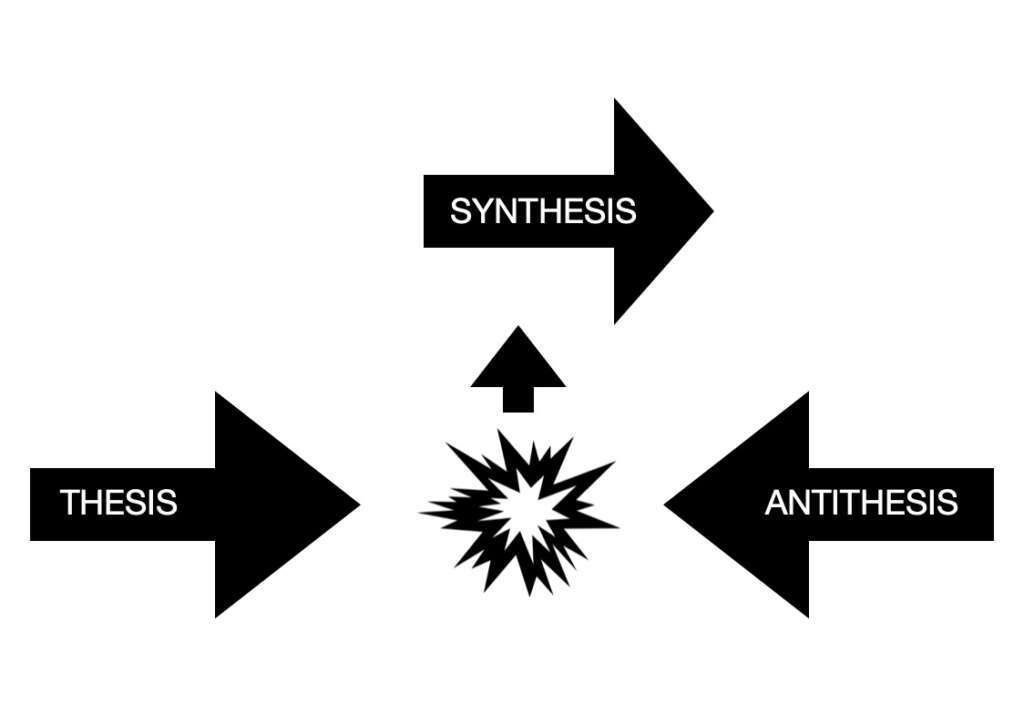
This reminds me of the dialect, a concept I once taught which is wrongfully credited to Hegel. Consider my diagram below, and I’ll explain it in a way that would positively horrify Hegel were he alive today.
The arrow marked “thesis” is a person moving through life, birth to old age. It could be you or me. The arrow marked “antithesis” is something unexpected that happens to him or her. It could be marriage, having a baby, winning the lotto or it could be a serious car accident, the death of a spouse, or an operation to correct a brain aneurysm that you never knew you had. When the two realities (thesis and antithesis) collide, a third, different or “hybrid” path or alternative arises, because the first two no longer exist. You are not the person you were in the thesis stage, because whatever you encountered changed your life for the better or the worse. So you must find a new way forward. One more example. You are living in a nice house near the beach and a hurricane blows it down. In other words, the thesis (your house) and the antithesis (the storm) collide. Now, a synthesis emerges. A new house, but decidedly different than the first one. Or, maybe your house wasn’t insured, and now you are homeless. There are all sorts of examples posssible. And just like the hypothetical person in the new home needs time to familiarize herself to where the closets are, what light switch works what light, a person who has had brain surgery, even something as seemingly trite as a stent has a new reality, and that must be explored as well. Yet, the downside of a clipping, coil or stent are certainly not as devestating as what might have happened had the aneurysm been left to rupture in its own course and time.
NOVEMBER 29, 2024 (F)
Wow! It’s been quite some time since I’ve added to this post. That’s good news for us, because it means that Deena’s recovery has been essentially unremarkable the past few months. No more episodes of scintillating scotoma, and a significant reduction in the number and severity of headaches as well. Last week she saw her neuro-surgeon and he seemed pleased as well. She’ll be on her blood thinner (Prasugrel) for another two months and then a second MR-Angiogram. And I’d like to add a caveat here on something called recanalization.)
I stumbled on this term recently and I was previously unfamilar with it. The medical definition is a bit complicated, but essentially it is possible for a coiled and/or stented intracranial aneurtsm to have a new lease on life, particularly if blood has been successful in entering the sac or pouch of the aneurysm for one reason or another, or if it the neck of the aneurysm was wider than usual. In fact, a larger aneurysm prior to surgery has a greater chance of presenting itself once a again as a health threat, though the odds are not necessarily significant (ceteris paribus, meaning all things equal.) As we read here:
“No other modifiable factors (elevated blood pressure, diabetes mellitus, or dyslipidemia) have been clearly associated with aneurysm recurrence after coiling. Several aneurysm factors are potentially or clearly associated with aneurysm recanalization after coiling such as wide neck and large and giant aneurysms . . .”
In other words, stopping smoking or controlling your blood pressure is important to ward against subsequent intracranial aneurysms from developing. But any effort you take seems to have no effect on the long term success (or not) of a treated aneurysm. So, what are the risks that you might need intervention once again if blood seeps into your treated aneurysm, causing it to resume increasing in size? According to Pathway, MD:
Recanalization rates vary depending on the treatment method and aneurysm characteristics.
A study involving 254 intracranial aneurysms treated with stent-assisted coiling reported recanalization rates of 8.0% and 13.5% for two different stent types.
Another study reported a recanalization rate of 26.4% in 91 aneurysms treated with endovascular coiling
A study of 236 aneurysms reported a recanalization rate of 14.0%
So, based on the studies above (which I can provide to anyone who requests them) the odds of someone needing additional intervention once an aneurysm has been coiled or treated with a stent are no more than one in four. Everyone else should e good.
Unless I uncorver additional material that seems worth mentioning, I may not check back in before Deena’s January MR-A. Happy Holidays, everyone!