NOTE: I have two additional aneurysm threads on this blog: How Deena recovered from her surgery here and additional information on intracranial aneurysms here.
One of the most important questions Deena and I had to ask of the other when we first met was whether we shared the same faith (or if any faith at all.) We could not at the time foresee my eventual cancer or Deena’s cerebral aneurysm. But having a mutual belief system meant that we had a common stratagem which we could fall back on when the road got bumpy (and as we were both approaching the age of seventy, the question was not if we would see health challenges but rather when.) Today, we learned about Omi’s aneurysm.
Economist Adam Smith wrote about an “invisible hand” in the marketplace. Looking back in my life, I saw many, many examples of where I was “nudged” a certain way by a similar such hand. For example, abandoning my short-lived career in logistics and retraining into the medical field in the Air Force when I was in my mid-twenties, and then taking—and later teaching—advanced courses in nursing and medicine to ER technicians and ICU staff. The result was that I could better care for my (now late) wife many years later when she faced multiple health issues. That was then. Today, I’m here for Deena.
The faith that Deena and I share has not immunized us from hardships or suffering in the past and, past being prologue, probably will not as we approach the future. C’est la vie. Christians may love and be loved by their Creator, but they don’t necessarily live charmed lives.
Deena had lost her husband Jim unexpectedly, and he was taken while he was in the prime of his life. Neither of us can understand or explain why. One might wonder where God was when Deena’s husband died? Or the week that my wife suffered multi-organ failure? In fact, God does not heal most people, or even many to my understanding or in my experience. But some people do go into remission from whatever they are suffering from. People occasionally wake up from comas, regain the use of atropied limbs, have malignant tumors reduced in size, recover the use of failing kidneys, survive stunning insults to their bodies from sepsis, car wrecks and gunshot wounds, or from falls, or wild animal attacks. In some cases, many people pray for those with diseases and disorder that they might recover. In other cases, not so and they may recover as well. The Bible says that God rains on the just and the unjust alike (Matthew 4:45.) More often than not, healing today is accomplished through medicine (the Apostle Luke, himself, was a physician.) Certainly, God does not need a physician to remove Deena’s aneurysm, but relying on someone of Luke’s profession is not a breach of faith. We believe that having been forewarned of it, we should use the common sense that God gave us and have it evaluated and treated. In Nehemiah 4:9, Gideon is quoted as saying “. . . we prayed to our God and posted a guard day and night to meet this threat.” Israel was about to be attacked by overwhelming forces. Gideon led his people in prayer, but then did the responsible thing by preparing for battle. Not everything in life is a test where a miracle is the solution. As Freud once said: “Sometimes a cigar is just a cigar.” The same is true of aneurysms. The professional literature tells us that as many as sixty percent of patients have an aneurysm which was not discovered because of misdiagnosis. These are people who sought out health care and medical advice, but ultimately succumbed because the warning signs of stroke were not properly interpreted or ignored. So, clearly, it is worthwhile, even critical, that a person (at least a person with risk factors) knows if he or she has an aneurysm. And that cannot be known without a CT scan or MRI.
When Deena first felt symptoms last Tuesday (restlessness, blurry vision, and a unusual sort of pain on the left side of her head) we checked her blood pressure and it was 189/111. That is well above normal as many of you can personally attest. As I drove her to Emergent Care (EC), I felt in my spirit that this was a warning, and that we should pay close attention to what followed. When she was being triaged at EC, she was asked if she thought this might be a stroke and she replied “Yes!” because her mom had suffered a deadly cerebral hemorrhage at age 45. Her mom smoked and also had hypertension, which are the two major risk factors for aneurysms. Deena never smoked, but she had hypertension nonetheless. So, they called an ambulance telling us they could not provide treatment given the answer Deena provided to them in response to their question. Arriving at the ER in an ambulance meant that Deena only needed to wait six hours to be moved to an inpatient area instead of the ten or twelve hours other patients had to wait to be treated (after triage.) During her wait in the ER, they called her for a CT-scan, an EKG and bloodwork. Had we tried to manage this at home, or on an outpatient basis, her aneurysm would have gone unnoticed, until . . .?
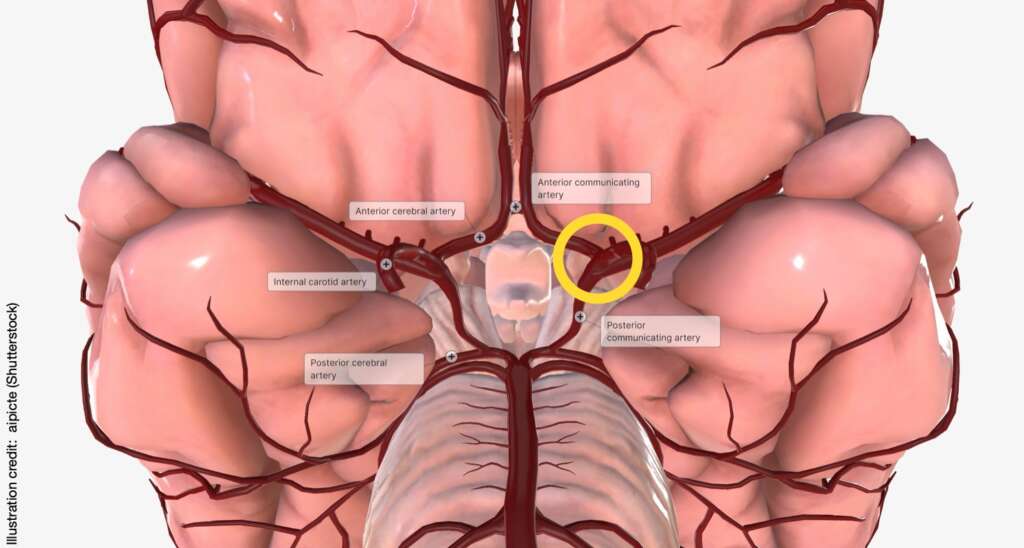
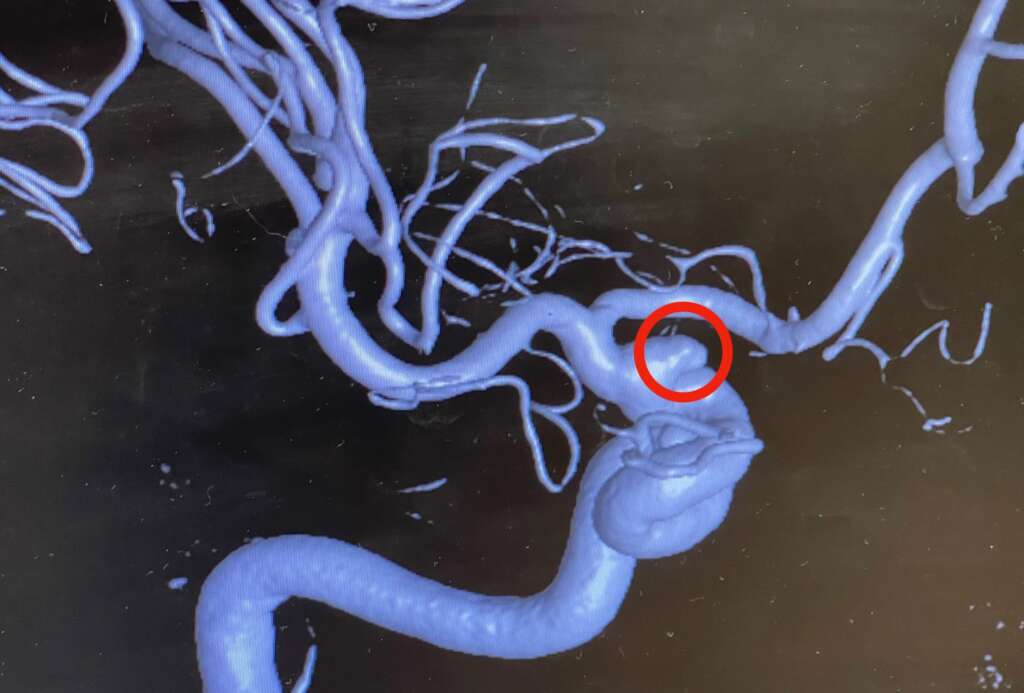
So, we had to wonder why God would reveal this potentially life-threatening defect to us unless it was to prompt us to some prudent action. That begins with prayer as Gideon noted. But that also includes a CT-angiogram and a visit with the neuro-surgeon next month as well. Deena is leaning towards getting the aneurysm removed, rather than living under a constant threat and I fully support her decision. God does not want people to live in fear. Deuteronomy 31:6 says “Do not be afraid or terrified . . .” This phrase or phrases very similar to it appear more often–some 365 times–in the Bible than any other phrase on any other topic! The surgery is safer than ever, but obviously there are risks which partly depend on how the OR team approaches the aneurysm, where the aneurysm is, the age and state of health of the patient, other comorbidities, etc. As far as I know from her CT report and the two neuro-surgeons and the hospitalist who spoke to us briefly while she was in the hallway of the hospital, the aneurysm is at the junction where her right internal carotid artery intersects the Circle of Willis at the base of Deena’s brain (see circled area in yellow on the diagram below.)
Thus, it may involve more than one blood vessel. But we don’t want to wait another year until a CT is repeated in June of 2025. By then, the aneurysm could be twice as large, leaking or ready to burst. Once a cerebral aneurysm of any size bursts, then all bets are off. Deena’s aneurysm is currently 5×7 mm. This, alone, makes Deena a good candidate for an invasive procedure to reduce/remove it.
What we’ve learned about aneurysms
Basically, “the term aneurysm is derived from the ancient Greek word aneurysma, which describes a widening.1” Civilization has known about aneurysms for more than 3,400 years.
In the fourteenth century B.C. the Egyptians . . .treated aneurysms by magico-religious therapies, but the nature and site of occurrence of these lesions are not mentioned nor the term applied to them.”
Aneurysms were first mentioned in the Eber’s Papyrus (written 1550 BC.) The great Roman physician Galen was the first to define and describe the disease, as he treated gladiators under the Coliseum in Rome and saw many aneurysms caused by trauma.
Causes of aneurysms
Smoking and hypertension are the main causes of aneurysms followed closely by trauma and hereditary. The role of nicotine in cigarettes is still uncertain:
There are multiple hypotheses about the mechanisms through which smoking can lead to vascular inflammation, hemodynamic stress, endothelial dysfunction, and, ultimately, wall weakening and rupture. Cigarettes are composed of a mixture of chemical substances that release a bunch of harmful toxins when burnt, which can enter into the bloodstream and lead to many vascular adverse effects. To understand it more clearly, we can analyze the impact of cigarette smoking on each stage of the development of aneurysms, such as its formation, growth, rupture, and, eventually, its recurrence.
The sheer force of blood driven though delicate blood vessels by high blood pressure can destroy them, particularly in the eyes, the kidneys and the brain. This is why hypertension is called “the silent killer.” Trauma (such as being driven against a seat belt in a motor vehicle accident can cause aneurysms in the arteries of your shoulder) or abdomen as can infections cause aneurysms as well. Then, there also seems to be a genetic predisposition.
Dr. Alejandro M. Spiotta of the University of South Carolina Medical Center notes speaking of the role of one parent or sibling with an aneurysm to another:
It’s really if you have two first degree relatives, but in my practice, if you have one and you are the second person, we’re not waiting for the third. So, if your mother and your sister had an aneurysm for example, we want to get you screened, we want to get all of your siblings screened and your children screened. I even go to aunts and uncles. And that can be by way of a CT angiogram, a CT-A or an MRA[Magnetic Resonance angiogram.] We’re not waiting for a third. And the big thing that I go over with patients is that I may be discussing you and now you are my patient, your family members are not my patients, so I cannot order that imaging study on them. So, the onus is on you as my patient to call them and say ‘Hey! I’m the third person down with an aneurysm and my neurosurgeon you all need to get screened.'”
Gender also plays a strong role with more aneurysms in women than in men. And these women are generally postmenopausal. This leads some investigators to wonder whether hormones such as estrogen play a role. However, women of any age can develop an aneurysm given the right causal factors (such as smoking and hypertension.)
Signs and symptoms of a cerebral aneurysm
The most common site for an aneurysm in the body is on the aorta, the great vessel that exits the heart with oxygenated blood. The second most common site is the brain. While there are different areas of the body and different types of aneurysms, I want to focus on the brain in this post to avoid confusion. And while there are many useful Youtube videos on aneurysms, the “go-to” resource for aneurysm of the brain is the Brain Aneurysm Foundation.
On the Brain Aneurysm Foundation’s website, you’ll learn that people with an unruptured aneurysm have the following signs and symptoms:
Blurred or double vision
A drooping eyelid
A dilated pupil
Pain above and behind one eye
Weakness and/or numbness
Once the aneurysm has ruptured, addition signs and symptoms may be present, including”
Sudden and severe headache, often described as “the worst headache of my life”
Nausea/vomiting
Stiff neck
Blurred or double vision
Sensitivity to light
Seizure
Drooping eyelid
A dilated pupil
Pain above and behind the eye
Loss of consciousness
Confusion
Weakness and/or numbness
If you experience any of these, you should have it evaluated immediately (STAT), even if it takes a 911 call.
Afterword
While our county has a teaching hospital with a good track record in aneurysm repair (according to our family doctor), Deena and I are considering traveling some distance from home to one of the top four or five treatment facilities in the country. Conventional wisdom says that if you need a major operation, you should choose a hospital where the procedure is a routine one, that is performed quite frequently. That way, you not only have skilled neurosurgeons but you have a more than competent OR team, post-op team and recovery team. Then, too it never hurts to get a second opinion. This is not unusual in medicine and doctors are quite professional about it.
GRATEFUL
I know Ron was hoping I would add a few words about my upcoming surgery to this blog, so I will attempt to explain the last few weeks and where I see myself in another month. Even though it was hard to hear, I am grateful they found my unruptured aneurysm. The night I got the diagnosis in the middle of the night, I shook life a leaf in late Autumn.
After all, I was lying on a tiny cot in the hallway at Albany Medical Center only 25 feet or so from where my own mother was lying in intensive care in 1970. I knew too well what her aneurysm did to her over the course of 4 months. It took her young life at almost 45 years of age.
Here I was over 54 years later, being asked if I wanted to have mine, fixed. “Squeeze my hands.” “Follow this pen with your eyes.” I wasn’t sure how improved the healthcare system in neurosurgery had progressed. Not getting it fixed was never an option these past six weeks for me, but the risks either way seemed so heavy.
I began to make a list of all the things that really mattered, like talking to family and friends and seeing them asap. I picked up my phone and made calls. My closest friends and family know, I do not call unless it’s VERY important. I prefer letters, text message and best of all face-to-face spending time with each other. That is why my kitchen is my lifeline. I love to hug and feed you. I was surprised how many of my friends reached out to me and many family members. As more details trickled out about how serious this brain aneurism is, I was flooded with support.
Ron got an unexpected kidney stone, so I needed to cancel a trip to surprise my oldest son for his 50th birthday and see many dear friends in Texas. I still hope and pray my son will come to New York; it’s been over a year since we had a weekend together in 2023. I miss him.
I finished my “Read this: after I am gone letters” right away. They were started in 2015, these are the hardest letters to ever write, yet I am glad I did this. Anxiety can really zap your energy and it has taken its toll on me. Every medical staff person I told always is shocked they found it, unruptured and many knew friends or patients who did not fair well, died, and or needed rehabilitation.
After meeting and talking to the neurosurgeon (who I did meet June 5 in ER) and looks a bit like Doogie Howser M.D., I am a bit more relieved, but still very nervous about the upcoming 3 D angiogram this week and surgery on August 9.
I know the Bible says, “Do not be afraid,” 365 times and I figure God understands we will be, so He reminds us so many times. My faith is strong, and I have asked God, to make it through, so I can get back to business taking care of Ron in his major health needs. Ron can’t read my expressions or my mind, so I tell him I’m okay most days and that’s how we roll. He’s a great guy who loves me dearly. He also told me he’d rather have cancer than an aneurysm, and I get that. We laughed, but inside I’m crying many days.
Thank you for every card, prayer, call and most of all visit. Time is my love language and you wanting to be with me is how I feel loved. Touch is another, so that’s why I hug often. I am so grateful. I can’t write letters to everyone I love, but if you are reading this and I am gone, I’m in a wonderful place with many loved ones who have passed before and there is absolutely no tears or pain and I’m happy. Forever.
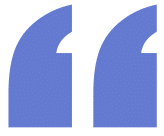
So, this (above) is what Deena’s stent looks like. I’m not a physician. I do wonder whether the mesh network of titanium “wires” is not to assist in the granualtion of the endothelial tissue of the artery? Like a lattice. When I used to debride second and third degree burns and other wounds, I was taught that providing a network of small “squares” on the raw surface of the burn or wound such as what specialized gauze might allow, is important to the regeneration of the tissue. If this holds true here, I suppose that in the weeks ahead, different “holes” at different places in the stent start developing new tissue. Just small spots here and there. Eventually, the individual squares of tissue start touching each other providing larger areas of tissue until finally, there is a continuous sheath of new, healthy, endothelial tissue with a good blood supply, etc.
Obviously, the stent is not as big as the photo. As we were sorting through Deena’s discharge paperwork yesterday, we came upon the same sort of ID “card” that one gets when they have a pacemaker implanted in their heart. The small ID paper–not even a card–had the manufacturer, the model and serial number of the stent on it as well as the date it was made. It might easily have been accidentially thrown away as it was not specifically explained during discharge. This information is most likely for recall purposes if the items in a certain lot number prove to be defective at some later date and need to be replaced. So, for those who ever need a stent (or a pacemaker), you’ll want to carry this card in your wallet or purse. And stents are used for different places in a patient’s body today, such as coronary arteries, renal and carotid arteries, and even arteries in the legs (anywhere there is a narrowing of the artery from plaque.) And, of course, they are used to repair cerebral aneurysms when clipping or coiling are not effective.
AUGUST 11, 2024 (S)
So, Deena is home resting after her discharge yesterday morning. It’s been two days since her stent was put in to seal off the aneurysm in her brain. Now that the chance of a leak or rupture has been mitigated, one issue remains: Keeping the stent functioning properly. This means keeping it in place, keeping it from allowing scar tissue to build up inside the stent that would narrow the artery (stenosis) and finally keeping blood clots from forming. Clots form for different reasons. In the case of a stent in an artery in the brain, a clot can form from the presence of a foreign body (the stent) in constant contact with the blood. So, patients like Deena need to be on blood thinners for at least six months after the stent is inserted to prevent clot formation. According to Harvard Health:
Stent thrombosis can happen at any time, but most clots form within the first month ofreceiving a stent. Skipping or stopping the anti-clotting medications is the biggest risk factorfor stent thrombosis.“
Aspirin needs to be taken daily for the rest of the patient’s life. The formation of a clot (thrombosis) in a stent would cause stroke-like symptoms, because the blood supply to the affected part of the brain would be deprived of blood.
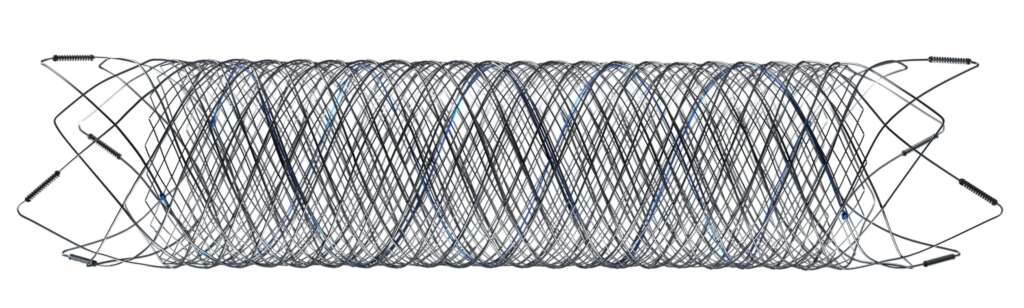
The other thing is that given the position of the stent in Deena’s brain, there is the posibility of transient visual disturbances. Two weeks ago, Deena experienced scintillating scotoma. While every person who has this describes it differently, the illustration below is a fair representatrion of what I see prior to a migraine. Parts of it may be similar to what Deena saw. In addition to the jagged lines, “popping” lights are also common. This resembles the bubbles children blow through a small circular applicator that is dipped in bubble soap and through which the child blows to form the bubbles. We can all recall the “popping” that occurs when these bubbles touch something.
What someone might see during an episode of scintillating scotoma.
The scintillating scotoma are thought by some researchers to be the consequence of insensible flow diversions of blood from one optic nerve to the other. The scotoma are typically harmless, though during the twenty or so minutes after they appear they cause profound changes to your vision until they resolve.
August 9, 2024 (F)
Our Hero: Deena’s Neuro Surgeon Dr. Nicholas Field.
Procedure was a complete success. Deena tolerated the stent placement well. She’s currently in recovery where she’ll remain until the endotrach tube is removed. She’ll spend the night in special care/intensive care while they do neuro checks and watch for bleeding at the femoral artery site. Then, home, with limited activities x four weeks.
Deena will remain on blood thinners for the rest of the year and on aspirin (82 mg/day) the rest of her life.
God be praised!
August 6, 2024 (T)
Last (Monday) night was difficult. Earlier that day, Deena’s potassium was again well below normal. That along with stress likely accounted for the bad headache which kept her awake until 4:30 a.m Tuesday morning. The smooth muscles in the blood vessels need potassium to relax, and this electrolyte was in short supply. As a result, her blood pressure was fairly high, but by itself, was not enough for a trip to the ER. However, the fact that there is one place known to have a weak spot in an artery in Deena’s body did not escape our notice.
Plus, for the first few days on BrilintaTM (a blood thinner), she had marked shortness of breath (SOB.) Even walking across the room was difficult. SOB is a common side effect which normally goes away after a few days on the drug. But because of it, her surgeon put her on yet a different blood thinner and by the time it arrived from the pharmacy yesterday afternoon, Deena was breathing easier. But by then, she was locked into this new anticoagulant, and for the initial dose, she had to take twelve pills! To me, you almost feel like you are caught in the current of the Niagara River rapidly approaching the Falls, but hoping you don’t drown before you get there (and that you don’t actually go over the falls, either.) You struggle to keep your head above the water, the sound and fury of the Falls becomes increasingly deafening, and your faith is definitely being tested. Fortunately, Deena has more than a few friends supporting her with letters, cards and encouraging comments.
Once they reach the aneurysm on Friday and insert the stent, repair the aneurysm, retrieve the catheter and plug up the hole in her femoral artery, then the main risk for harm is a blood clot forming in or around the stent. This risk exists with coronary stents as well. So, while blood thinners work in different ways, the strategy is to make it more difficult for blood to clot, either by increasing the time needed to clot, interferring with platelets in the blood, etc. Maintaining a therapeutic level or anticoagulants in her blood will be vital during the next five months until the stent starts to endothelialize, the medical term used to descibe a thin coating of normal body tissue that glazes the titanium surface of the stent. At that point, the clot (stroke) risk is minimum, though Deena will have to take 82 mg of aspirin each day for the rest of her life. That alone might be useful in preventing a clot elsewhere in her body, such as in the arteries of her heart, the veins in her legs, etc.
Whoever said that life was easy?
August 2, 2024 (F)
Less that a week to go before surgery. But there are a couple of glitches. Deena’s potassium (K) has dropped below 3.0 again (anything below 3.5 is low.). So, they are increasing her p.o. (oral) potassium. Because potassium is critical for heart function, an anesthesiologist will probably not want to operate unless they can raise it before Friday. I told Deena that in the “old days” when I worked in USAF hospitals, they would bring her in the day before and hang an IV drip with potassium added to get her ready. But today, dozens (or more) beds in the local regional hospital go empty because there are not enough nurses to staff them, hence there is a bed “shortage.” Also, her anticoagulation level is not high enough for surgery. They need to further reduce the number of platelets in her blood before Friday, less a clot form around the stent. So, they started Deena on a new anticoagulant.
She also has some other blood dyscrasias with high leves of monocytes, basophils and eosinophils which usually indicate infection or inflammation. Stress is another possibility. More blood to be drawn on Tuesday.
July 19, 2024 (F)
Deena had her MRA (Magnetic Resonance Angiogram) today. It went smoothly overall using her right radial artery at the wrist for portal entry. After a pre-op cocktail of Midazolam and Fentanyl, Deena was pretty zonked out, though she could hear bits and pieces of conversations, as well as vaguely feel the retraction of the probe as it exited her brain and returned to her wrist. Her three hours or so in recovery consisted of checking her vital signs and running neuro assessments, plus attending to the inflatable pressure dressing on her wrist and starting her on food and fluids again.
A photo of Deena’s aneurysm (circled) which we saw on Wednesday, July 24th as the neurosurgeon finalized his preparation instructions. The large artery at the bottom is the right carotid artery.The other branch-like structures are minor arteries of that region of the brain.
However, as soon as she was discharged and we returned home, she experienced what is known as scintillating scotoma, which some people (including myself) experience as an aura prior to a migraine. Everyone’s perception is different. Deena and I both saw “popping” lights (like a soap bubble popping) and they generally resolve within twenty minutes or so. Mine are like Moire patterns. But in any event, they make it impossible to read or function. Deena’s blood pressure was normal, and her pupils were normal. She was oriented to time and place, though counting backwards from 100 by 7 is a challenge regardless of any person’s level of consciousness. She did have a headache, and as it as afterhours, we went to the ER where they contacted her surgeon. He thought it might have been the effects of the contrast and the shock of the experience to her brain. So, we returned home and there were no more issues.
Deena will be placed on a blood thinner this week in anticipation of the surgery. She will remain on it until the end of the year. By that time, the interior of the stent will have acquired a thin layer of epithelial-like tissue, which means the titanium in the stent is no longer directly exposed to the platelets in the blood. Clots tend to form around exposed metallic stents, mechanical heart valves, etc.
The surgeon feels comfortable with the surgery and we’re good to go. Only sixteen days to go.
July 12, 2024 (F)
Deena had a pulmonary function test scheduled for today. When we arrived at the clinic and they understood that she had an intracranial aneurysm which was ripe for surgery, they declined to perform the test, stating that there was a chance that the procedure could in some cases cause a cerebral hemmorhage to burst. Likewise, other activities such as performing a valsalvar maneuver (pinching your nose while breathing out as one does on an aircraft to equalize pressure or before or after diving), bearing down while on the toilet, sexual activity, events that cause one’s blood pressure to suddenly peak all appear to be precursors to a possible rupture. This was news to me, as I have had limited experience dealing with stroke patients and those with other similar events (such as aneurysms.) Nor is there very much in the literature.
July 11, 2024 (R)
Image credit: farakos (iStock.)
Events and details are picking up speed and the last pieces of the puzzle are starting to fall into place. Now that Deena has an OR date, we are hearing daily about what needs to be done and how soon to must be accomplished. This past Wednesday, Deena had a chest X-ray which was normal in spite of her past diagnosis of Alpha-1 antitrypsin (AAT) deficiency. This is no doubt in part due to the fact that she has never smoked. She was also scheduled for a pulmonary function test (PFT) tomorrow afternoon, but she seems well enough for surgery as far as that system goes. We read the notes of her visit with the neurosurgeon two days ago and without doing a formal assessment of her cranial nerves, he did do an informal cognitive and functional assessment on Deena and he seems convinced of her robust health. Not everybody is eligible for every procedure. For example, someone with a history of noncompliance with their doctor’s orders in the past might not receive a liver transplant. Certain mental health issues or co-mobidities (i.e., other significant or terminal diseases or disorders) might disqualify someone from surgery.
We are also encouraged by some of the scheduling assistants we have met. These key personnel are the ones who can make the experience run smoothly. Occasionally, they serve as gatekeepers to the physicians, and they can elevate a patient’s rank when resources and the surgical schedule seems particularly challenging (as it is today.)
Deena also got a call from the surgeon’s office concerning blood work needed before her CT angiogram next week. This particularly involves her creatinine level, a indice of her kidney function. Deena’s creatinine has been well within normal limits in the past is is likely so now. However, radiological exams involving contrast can in 2% of the cases temporarily depress kidney function in the short term and in some ever rarer cases, shut the kidneys down.2 A future concern as the OR date approaches is her Prothrombin time:
(PT) is a blood test that measures the time it takes for the liquid portion (plasma) of your blood to clot. It measures the function of a part of the clotting system. A related blood test is partial thromboplastin time (PTT), which measures the function of a different part of the clotting system.”
Blood that fails to clot promptly (within parameters) or which clots too easily are equally problematic before, during and after surgery.
Today, we went to the gym where Deena swam several laps in the pool to boost her stamina.
July 10, 2024 (W)
We saw Deena’s neurosurgeon today. Deena has a saccular aneurysm which is defined as a brain aneurysm, which “happens when a sac or pouch forms on one side of the blood vessel wall.” The neurosurgeon took us through the CT images to show it to us. He said there were several options available:
Deena could wait and just have annual scans done to see if the aneurysm changes in size or shape.
She could have a cerebral angiogram or MRA (Magnetic Resonance Angiogram) to better understand it and decide where and how to go from there.
She could a cerebral angiogram immediately before general anesthesia was induced on the day of surgery.
We did not need to insist on surgery, because the surgeon recommended it as the most prudent course of action given her family history and the size of the aneurysm. We chose the second of these options.
The surgeon also mentioned finding a second, smaller aneurysm in the cavernous sinus which is of no immediate concern because of its size and location. But it is the first we heard of this
Because of the shape of Deena’s aneurysm, and particularly because of its wide neck where it separates from the artery, neither a clip nor a coil would work well. The surgeon proposed inserting a shunt in the artery which would be of metal, and because it is of metal, Deena would need to be on blood thinners for at least the remainder of this year, since these kind of shunts can lead to blood clot formation.
So, Deena has been scheduled for an MRA a week from Friday. Her surgery will be on Friday, August 9th. At some point between those two dates, her surgeon will meet with her to explain the details of the procedure. She will need one or two nights in the hospital after surgery and before discharge.
A second appointment today with the pulmonary lab seemed to confirm her diagnosis of Alpha-1 antitrypsin (AAT) deficiency. “Alpha Trip” as it is called is an genetic autosomal co-dominant disorder, meaning it can be expressed either as a mild disorder as in Deena’s case or as a severe, life threatening disorder (such as the one that took the life of her brother.) All things equal, Alpha Trip should not in itself keep Deena from enjoying a long, healthy life, especially since she does not smoke. But our questions are whether it poses a challenge for the anesthesiologist as he inturbates her during surgery.
So, a trip to New York University (NYU) seems to be off the table because we are moving ahead fairly rapidly up here in Albany while we have heard nothing from NYU since they received her records. The surgeon seems competent and assuring enough and we have no leading at the moment to look elsewhere.
July 2, 2024 (T)
Approximate position of Deena’s aneurysm, but closer to the base of the brain. Conceptual image, 3D illustration. Credit Kateryna Kon (Shutterstock.)
While waiting for Deena’s appointment with the local neurosurgeon a week from tomorrow, we also sent her records to New York University’s Langone’s Center for Stroke and Neurovascular Diseases which is located in mid-Manhattan just south of the United Nations. We understand that Medicare authorizes second opinions and there is no referral needed. The Langone Center has an outstanding track record in cerebral aneurysm repair, and we already have a neurosurgeon in mind at the Center. After visiting each of the two surgeons (local and in NY City, she will decide–with my full support–where to have the procedure done. We’ll be in the City tomorrow and will likely give the NYU facility a quick once over if possible.
The Brain Aneurysm Foundation has numerous personal stories from people who have had ruptured brain aneurysms. An interesting story of a woman who had a cerebral aneurysm rupture while on a Microsoft Teams conference can be found here.
June 24, 2024 (M)
Wrote a post today called Synchronicity that describes some of the recent events that are preparing Deena psychologically and spiritually for surgery should that be necessary. Meanwhile, we continue to make arrangements in our affairs to prepare for any eventuality.
June 22, 2024 (S):
Deena has an appointment to see her eye doctor in the next week or two. She has intermittent issues with bluriness and she is more photophobic (sensitive to bright light) than ever. The results of her eye exam when contrasted to the ones in the past might indicate if there is a problem brewing, and her surgeon would welcome the test because regardless of the findings, it would be another piece of the puzzle. Sometimes there is a collapse in a person’s peripheral vision and changes in the pupillary response.
June 20, 2024 (R):
We went to the Department of Neurosurgey with a folder with well more than a hundred Magnetic Resonance Imaging (MRI) photos of her cerebrum from 2015. Dee had this done in Texas when she lost most of her sense of smell. We’re not expecting the 2015 MRI to show an aneurysm, else the radiologist in Texas would have caught it. So, her aneurysm not very old as far as aneurysms go. We also submitted a narrative summary of what we want the doctor to know. She has several risk factors, including lifelong hypertension, a mother who died at 45 from an intracranial hemorrhage and a brother who had a cerebral aneurysm, himself. Our summary also included symptoms that might be useful to the surgeon. At the very least, the 2015 MRI is a baseline moving forward. It was a relief to visit the Neurosurgery office to see where we’ll be visiting for her appointment, just nineteen days from now.
FOOTNOTES
1Krajíček, Milan, et al. “ANEURYSMS.” Cardiovascular Surgery, Karolinum Press, 2014, pp. 219–35. JSTOR, https://doi.org/10.2307/j.ctv371cpm7.17. Accessed 12 June 2024.
2Contrast induced nephropathy (CIN) is a rare disorder and occurs when kidney problems are caused by the use of certain contrast dyes. In most cases contrast dyes used in tests, such as CT (computerized tomography) and angiograms, have no reported problems. About 2 percent of people receiving dyes can develop CIN. However, the risk for CIN can increase for people with diabetes, a history of heart and blood diseases, and chronic kidney disease (CKD). For example, the risk of CIN in people with advanced CKD (glomerular filtration rate (GFR) below 30 mL/min/1.73m2), increases to 30 to 40 percent. The risk of CIN in people with both CKD and diabetes is 20 to 50 percent.
CIN is associated with a sharp decrease in kidney function over a period of 48-72 hours. The symptoms can be similar to those of kidney disease, which include feeling more tired, poor appetite, swelling in the feet and ankles, puffiness around the eyes, or dry and itchy skin. In many cases, CIN is reversible and people can recover. However, in some cases, CIN can lead to more serious kidney problems and possible heart and blood vessel problems.